

Hernia recurrence as a problem of biology and collagen
- PMID: 21187987
- PMCID: PMC2999776
- DOI: 10.4103/0972-9941.27729
Hernia recurrence as a problem of biology and collagen
Abstract
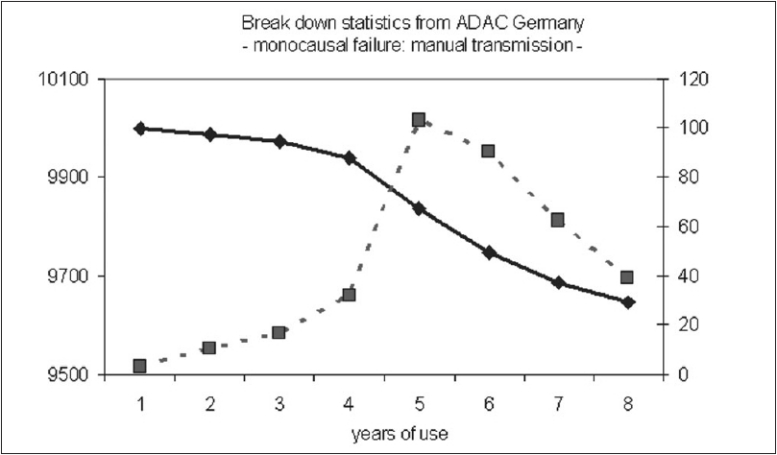
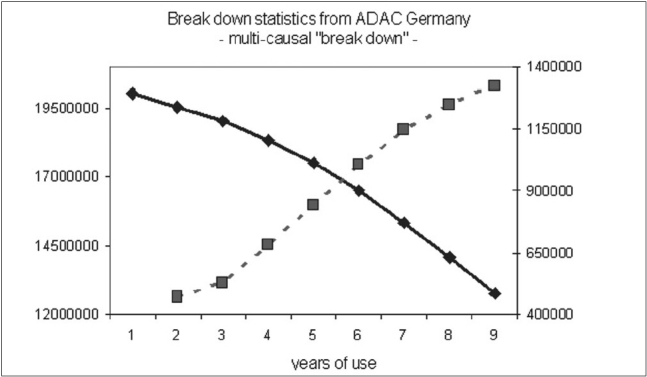
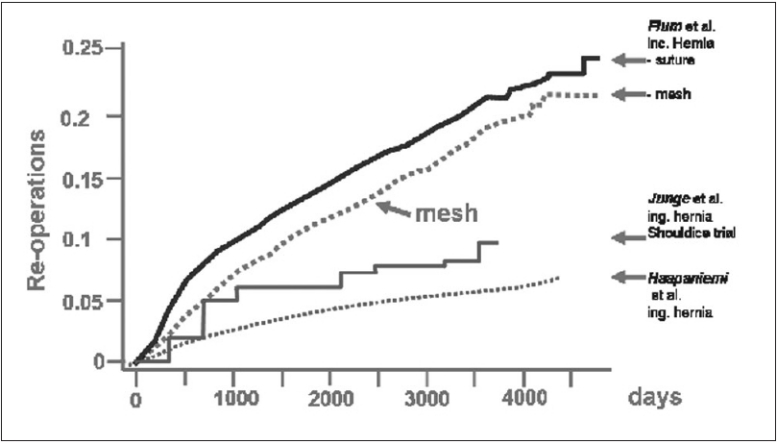
Usually an abdominal wall hernia is regarded as a mechanical problem with a local defect which has to be closed by technical means. Despite the introduction of several therapeutic improvements, recurrent hernias still appear in 10-15%. Therefore, reasons for a recurrence are discussed in a more fundamental way. It is assumed that a failure mainly depends on the quality of the repair. Correspondingly, in principle, the close causal relationship between the technical component and its failure during time is reflected by an s-shaped outcome curve. In contrast, the configuration of the outcome curve changes markedly if a breakdown is caused by numerous components. Then, the superposition of all incidence curves inevitably leads to a linear decline of the outcome curve without any s-shaped deformation. Regarding outcome curves after hernia repair, the cumulative incidences for recurrences of both incisional and inguinal hernia show a linear rise over years. Considering the configuration of outcome curves of patients with hernia disease, it may therefore be insufficient to explain a recurrence just by a failing technical repair. Rather, biological reasons should be suspected, such as a defective wound healing with impaired scarring process. Recent molecular-biological findings provide increasing evidence of underlying biochemical alterations in patients with recurrent hernia. Until predicting markers to identify patients with an impaired wound healing are available and considering the formation of insufficient scar as the underlying disease, the consequences for every surgical repair should be a supplementary reinforcement with nonabsorbable alloplastic nets as flat meshes with an extensive overlap.
Keywords: Biology; collagen; hernia; network; recurrence; wound healing.
Conflict of interest statement
Figures
References
-
- Conze J, Prescher A, Klinge U, Saklak M, Schumpelick V. Pitfalls in retromuscular mesh repair for incisional hernia: The importance of the “fatty triangle”. Hernia. 2004;8:255–9. - PubMed
-
- Israelsson LA, Smedberg S, Montgomery A, Nordin P, Spangen L. Incisional hernia repair in Sweden 2002. Hernia. 2006;10:258–61. - PubMed
-
- Conze J, Klinge U, Schumpelick V. Incisional hernia. Chirurg. 2005;76:897–909. - PubMed
-
- Amid PK, Lichtenstein IL. Retromuscular alloplasty of large scar hernias: A simple staple attachment technique. Chirurg. 1996;67:648–52. - PubMed
-
- Schumpelick V, Klinge U, Welty G, Klosterhalfen B. Meshes within the abdominal wall. Chirurg. 1999;70:876–87. - PubMed
LinkOut - more resources
Full Text Sources