

Predictive value of plasma galectin-3 levels in heart failure with reduced and preserved ejection fraction
- PMID: 21189092
- PMCID: PMC3028573
- DOI: 10.3109/07853890.2010.538080
Predictive value of plasma galectin-3 levels in heart failure with reduced and preserved ejection fraction
Abstract
Aims: galectin-3 is an emerging biomarker which has been studied in relatively small heart failure (HF) cohorts with predominantly systolic HF. We studied the prognostic value of base-line galectin-3 in a large HF cohort, with preserved and reduced left ventricular ejection fraction (LVEF), and compared this to other biomarkers.
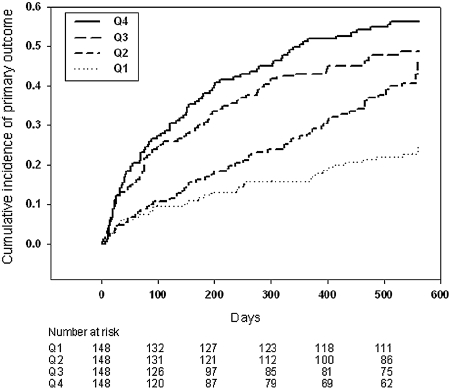
Methods: we studied 592 HF patients who had been hospitalized for HF and were followed for 18 months. The primary end-point was a composite of all-cause mortality and HF hospitalization.
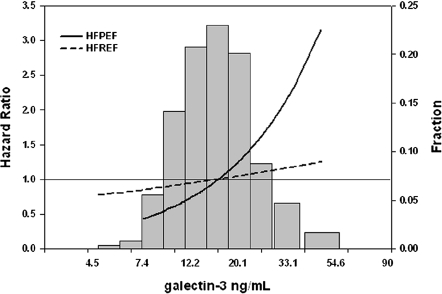
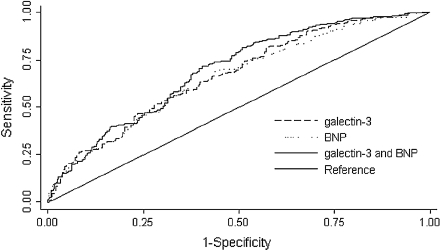
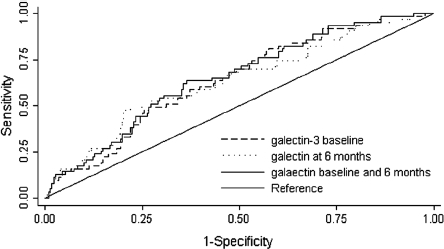
Results: a doubling of galectin-3 levels was associated with a hazard ratio (HR) of 1.97 (1.62-2.42) for the primary outcome (P < 0.001). After correction for age, gender, BNP, eGFR, and diabetes the HR was 1.38 (1.07-1.78; P = 0.015). Galectin-3 levels were correlated with higher IL-6 and CRP levels (P < 0.002). Changes of galectin-3 levels after 6 months did not add prognostic information to the base-line value (n = 291); however, combining plasma galectin-3 and BNP levels increased prognostic value over either biomarker alone (ROC analysis, P < 0.05). The predictive value of galectin-3 was stronger in patients with preserved LVEF (n = 114) compared to patients with reduced LVEF (P < 0.001).
Conclusions: galectin-3 is an independent marker for outcome in HF and appears to be particularly useful in HF patients with preserved LVEF.
Figures
References
-
- Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P, Poole-Wilson PA, et al. for ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM) Eur Heart J. 2008;29:2388–442. - PubMed
-
- De Boer RA, Voors AA, Muntendam P, van Gilst WH, van Veldhuisen DJ. Galectin-3: a novel mediator of heart failure development and progression. Eur J Heart Fail. 2009;11:811–7. - PubMed
-
- Yang RY, Rabinovich GA, Liu FT. Galectins: Structure, function and therapeutic potential. Expert Rev Mol Med. 2008;13:e17–39. - PubMed
-
- Sharma UC, Pokharel S, van Brakel TJ, van Berlo JH, Cleutjens JP, Schroen B, et al. Galectin-3 marks activated macrophages in failure-prone hypertrophied hearts and contributes to cardiac dysfunction. Circulation. 2004;110:3121–8. - PubMed
-
- van Kimmenade RR, Januzzi JL, Jr, Ellinor PT, Sharma UC, Bakker JA, Low AF, et al. Utility of amino-terminal pro-brain natriuretic peptide, galectin-3, and apelin for the evaluation of patients with acute heart failure. J Am Coll Cardiol. 2006;48:1217–24. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous