

Guidelenines in the management of obstructing cancer of the left colon: consensus conference of the world society of emergency surgery (WSES) and peritoneum and surgery (PnS) society
- PMID: 21189148
- PMCID: PMC3022691
- DOI: 10.1186/1749-7922-5-29
Guidelenines in the management of obstructing cancer of the left colon: consensus conference of the world society of emergency surgery (WSES) and peritoneum and surgery (PnS) society
Abstract
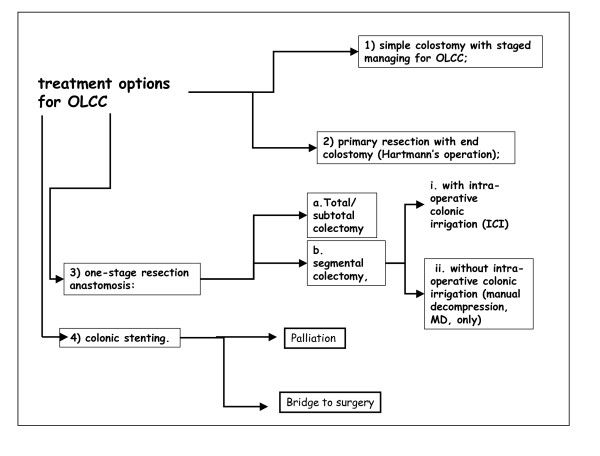
Background: Obstructive left colon carcinoma (OLCC) is a challenging matter in terms of obstruction release as well of oncological issues. Several options are available and no guidelines are established. The paper aims to generate evidenced based recommendations on management of OLCC.
Methods: The PubMed and Cochrane Library databases were queried for publications focusing on OLCC published prior to April 2010. A extensive retrieval, analyses, and grading of the literature was undertaken. The findings of the research were presented and largely discussed among panellist and audience at the Consensus Conference of the World Society of Emergency Surgery (WSES) and Peritoneum and Surgery (PnS) Society held in Bologna July 2010. Comparisons of techniques are presented and final committee recommendation are enounced.
Results: Hartmann's procedure should be preferred to loop colostomy (Grade 2B). Hartmann's procedure offers no survival benefit compared to segmental colonic resection with primary anastomosis (Grade 2C+); Hartmann's procedure should be considered in patients with high surgical risk (Grade 2C). Total colectomy and segmental colectomy with intraoperative colonic irrigation are associated with same mortality/morbidity, however total colectomy is associated with higher rates impaired bowel function (Grade 1A). Segmental resection and primary anastomosis either with manual decompression or intraoperative colonic irrigation are associated with same mortality/morbidity rate (Grade 1A). In palliation stent placement is associated with similar mortality/morbidity rates and shorter hospital stay (Grade 2B). Stents as a bridge to surgery seems associated with lower mortality rate, shorter hospital stay, and a lower colostomy formation rate (Grade 1B).
Conclusions: Loop colostomy and staged procedure should be adopted in case of dramatic scenario, when neoadjuvant therapy could be expected. Hartmann's procedure should be performed in case of high risk of anastomotic dehiscence. Subtotal and total colectomy should be attempted when cecal perforation or in case of synchronous colonic neoplasm. Primary resection and anastomosis with manual decompression seems the procedure of choice. Colonic stents represent the best option when skills are available. The literature power is relatively poor and the existing RCT are often not sufficiently robust in design thus, among 6 possible treatment modalities, only 2 reached the Grade A.
Similar articles
-
2017 WSES guidelines on colon and rectal cancer emergencies: obstruction and perforation.World J Emerg Surg. 2018 Aug 13;13:36. doi: 10.1186/s13017-018-0192-3. eCollection 2018. World J Emerg Surg. 2018. PMID: 30123315 Free PMC article. Review.
-
Emergency management of malignant acute left-sided colonic obstruction.Ann R Coll Surg Engl. 2008 Apr;90(3):181-6. doi: 10.1308/003588408X285757. Ann R Coll Surg Engl. 2008. PMID: 18430330 Free PMC article. Review.
-
Reviewing the Management of Obstructive Left Colon Cancer: Assessing the Feasibility of the One-stage Resection and Anastomosis After Intraoperative Colonic Irrigation.Clin Colorectal Cancer. 2017 Jun;16(2):e89-e103. doi: 10.1016/j.clcc.2016.12.001. Epub 2017 Jan 18. Clin Colorectal Cancer. 2017. PMID: 28254356
-
Emergency management of acute colonic cancer obstruction.J Visc Surg. 2012 Feb;149(1):e3-e10. doi: 10.1016/j.jviscsurg.2011.11.003. Epub 2011 Dec 19. J Visc Surg. 2012. PMID: 22189474 Review.
-
Management of malignant left colonic obstruction: is an initial temporary colostomy followed by surgical resection a better option?Colorectal Dis. 2013 Nov;15(11):e646-53. doi: 10.1111/codi.12335. Colorectal Dis. 2013. PMID: 23819886
Cited by
-
A prospective evaluation of short-term and long-term results from colonic stenting for palliation or as a bridge to elective operation versus immediate surgery for large-bowel obstruction.Surg Endosc. 2013 Mar;27(3):832-42. doi: 10.1007/s00464-012-2520-0. Epub 2012 Oct 6. Surg Endosc. 2013. PMID: 23052501
-
Acute PresentatiOn of coLorectaL cancer - an internatiOnal snapshot (APOLLO): Protocol for a prospective, multicentre cohort study.Colorectal Dis. 2023 Jan;25(1):144-149. doi: 10.1111/codi.16464. Epub 2023 Jan 16. Colorectal Dis. 2023. PMID: 36579365 Free PMC article.
-
Self-Expandable Metal Stents for Colorectal Cancer: From Guidelines to Clinical Practice.GE Port J Gastroenterol. 2016 Oct 4;23(6):293-299. doi: 10.1016/j.jpge.2016.06.003. eCollection 2016 Nov-Dec. GE Port J Gastroenterol. 2016. PMID: 28868482 Free PMC article.
-
The factors that affect the mortality of emergency operated ASA 3 colon cancer patients.Pan Afr Med J. 2020 Aug 17;36:290. doi: 10.11604/pamj.2020.36.290.24385. eCollection 2020. Pan Afr Med J. 2020. PMID: 33117484 Free PMC article.
-
Treatment of colorectal cancer in older patients.Nat Rev Gastroenterol Hepatol. 2012 Dec;9(12):716-25. doi: 10.1038/nrgastro.2012.196. Epub 2012 Oct 9. Nat Rev Gastroenterol Hepatol. 2012. PMID: 23045000 Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
