

Intradermal vaccinations with RNA coding for TAA generate CD8+ and CD4+ immune responses and induce clinical benefit in vaccinated patients
- PMID: 21189474
- PMCID: PMC3098631
- DOI: 10.1038/mt.2010.289
Intradermal vaccinations with RNA coding for TAA generate CD8+ and CD4+ immune responses and induce clinical benefit in vaccinated patients
Abstract
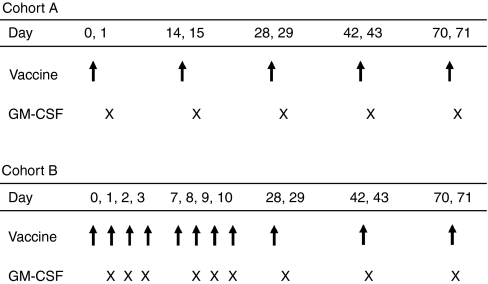
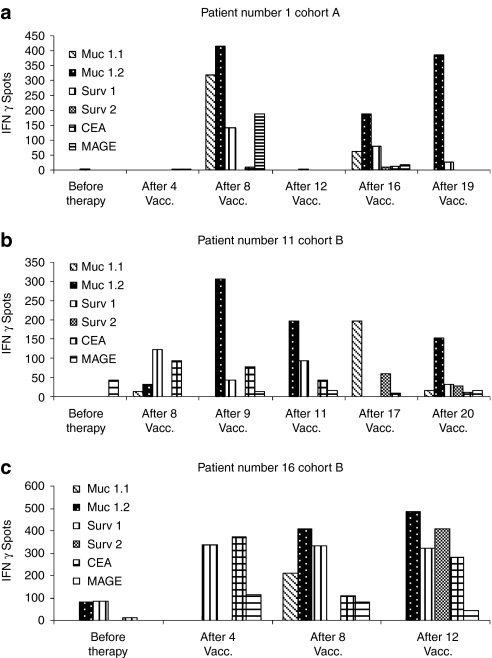
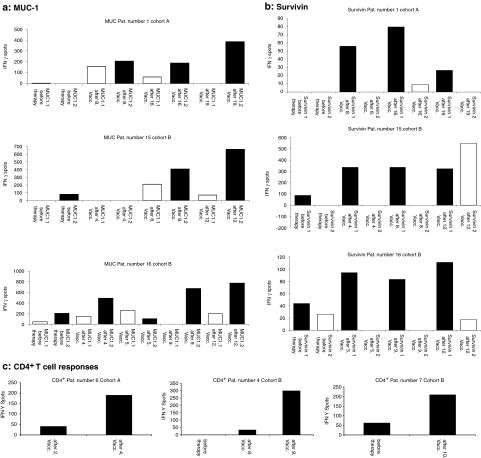
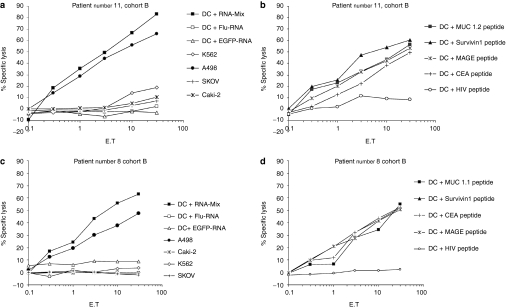
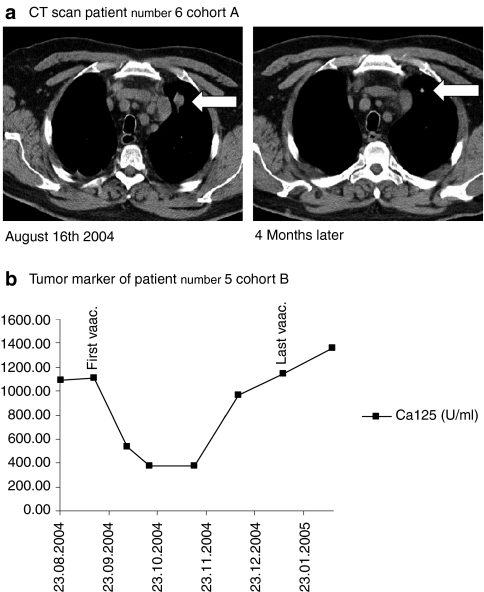
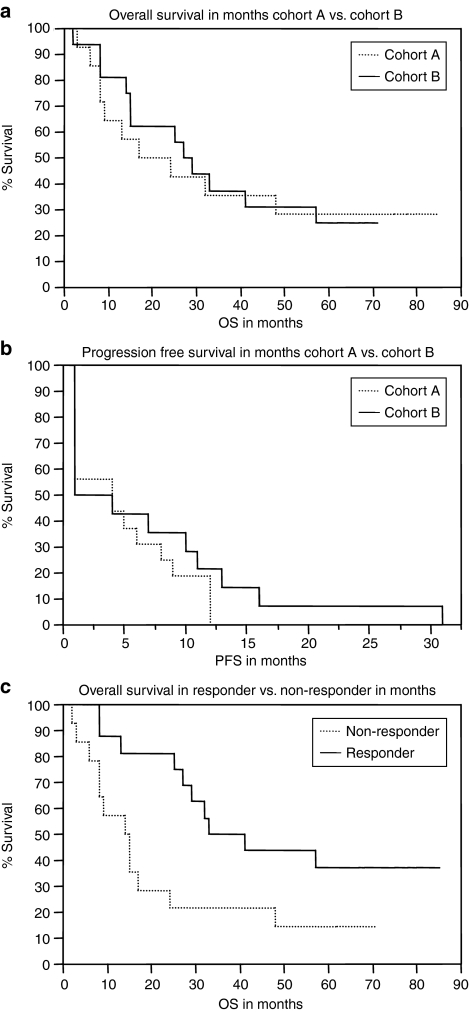
The aim of this phase I/II nonrandomized trial was to assess feasibility, safety as well as immunological and clinical responses of a mRNA-based vaccination in patients with stage IV renal cell cancer using granulocyte-macrophage colony stimulating factor (GM-CSF) as adjuvant. Intradermal injections of in vitro transcribed naked mRNA, which was generated using plasmids coding for the tumor-associated antigens mucin 1(MUC1), carcinoembryonic (CEA), human epidermal growth factor receptor 2 (Her-2/neu), telomerase, survivin, and melanoma-associated antigen 1 (MAGE-A1) were performed in 30 enrolled patients. In the first 14 patients (cohort A) vaccinations were administered on days 0, 14, 28, and 42 (20 µg/antigen) while in the consecutive 16 patients (cohort B) an intensified protocol consisting of injections at days 0-3, 7-10, 28, and 42 (50 µg/antigen) was used. In both cohorts, after this induction period, vaccinations were repeated monthly until tumor progression analyzed by Response Evaluation Criteria In Solid Tumors criteria (RECIST). Vaccinations were well tolerated with no severe side effects and induced clinical responses [six stable diseases (SD) and one partial response in cohort A and nine SD in cohort B]. In cohort A, 35.7% survived 4 years (median survival 24 months) compared to 31.25% in cohort B (median survival 29 months). Induction of CD4(+) and CD8(+) T cell responses was shown for several tumor-associated antigens (TAA) using interferon-γ (IFN-γ) enzyme-linked immunosorbent spot (ELISpot) and Cr-release assays.
Figures
References
-
- Motzer RJ, Bander NH., and, Nanus DM. Renal-cell carcinoma. N Engl J Med. 1996;335:865–875. - PubMed
-
- Belldegrun A, Muul LM., and, Rosenberg SA. Interleukin 2 expanded tumor-infiltrating lymphocytes in human renal cell cancer: isolation, characterization, and antitumor activity. Cancer Res. 1988;48:206–214. - PubMed
-
- Thurnher M, Radmayr C, Ramoner R, Ebner S, Böck G, Klocker H, et al. Human renal-cell carcinoma tissue contains dendritic cells. Int J Cancer. 1996;68:1–7. - PubMed
-
- Michael A., and, Pandha HS. Renal-cell carcinoma: tumour markers, T-cell epitopes, and potential for new therapies. Lancet Oncol. 2003;4:215–223. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
