Obstructive sleep apnea syndrome in children: Epidemiology, pathophysiology, diagnosis and sequelae
- PMID: 21189956
- PMCID: PMC3004499
- DOI: 10.3345/kjp.2010.53.10.863
Obstructive sleep apnea syndrome in children: Epidemiology, pathophysiology, diagnosis and sequelae
Abstract
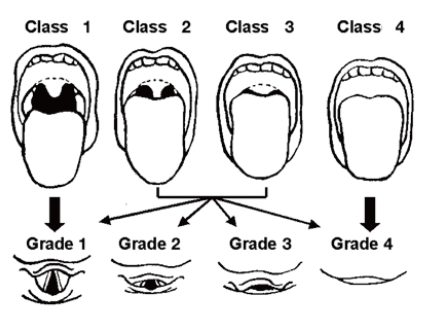
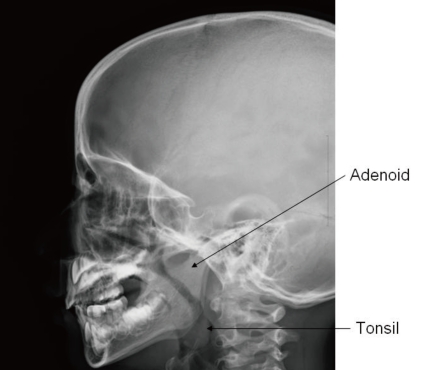
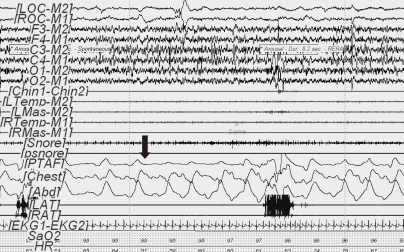
The prevalence of pediatric obstructive sleep apnea syndrome (OSAS) is approximately 3% in children. Adenotonsillar hypertrophy is the most common cause of OSAS in children, and obesity, hypotonic neuromuscular diseases, and craniofacial anomalies are other major risk factors. Snoring is the most common presenting complaint in children with OSAS, but the clinical presentation varies according to age. Agitated sleep with frequent postural changes, excessive sweating, or abnormal sleep positions such as hyperextension of neck or abnormal prone position may suggest a sleep-disordered breathing. Night terror, sleepwalking, and enuresis are frequently associated, during slow-wave sleep, with sleep-disordered breathing. Excessive daytime sleepiness becomes apparent in older children, whereas hyperactivity or inattention is usually predominant in younger children. Morning headache and poor appetite may also be present. As the cortical arousal threshold is higher in children, arousals are not easily developed and their sleep architectures are usually more conserved than those of adults. Untreated OSAS in children may result in various problems such as cognitive deficits, attention deficit/hyperactivity disorder, poor academic achievement, and emotional instability. Mild pulmonary hypertension is not uncommon. Rarely, cardiovascular complications such as cor pulmonale, heart failure, and systemic hypertension may develop in untreated cases. Failure to thrive and delayed development are serious problems in younger children with OSAS. Diagnosis of pediatric OSAS should be based on snoring, relevant history of sleep disruption, findings of any narrow or collapsible portions of upper airway, and confirmed by polysomnography. Early diagnosis of pediatric OSAS is critical to prevent complications with appropriate interventions.
Keywords: Child; Epidemiology; Obstructive sleep apnea syndrome; Pathophysiology; Sequelae.
Figures
References
-
- American Thoracic Society. Standards and indications for cardiopulmonary sleep studies in children. Am J Respir Crit Care Med. 1996;153:866–878. - PubMed
-
- Marcus CL. Sleep-disordered breathing in children. Curr Opin Pediatr. 2000;12:208–212. - PubMed
-
- Fiorino EK, Brooks LJ. Obesity and respiratory diseases in childhood. Clin Chest Med. 2009;30:601–608. x. - PubMed
-
- Benninger M, Walner D. Obstructive sleep-disordered breathing in children. Clin Cornerstone. 2007;9(Suppl 1):S6–S12. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials