

Obstetric outcomes after treatment of periodontal disease during pregnancy: systematic review and meta-analysis
- PMID: 21190966
- PMCID: PMC3011371
- DOI: 10.1136/bmj.c7017
Obstetric outcomes after treatment of periodontal disease during pregnancy: systematic review and meta-analysis
Abstract
Objective: To examine whether treatment of periodontal disease with scaling and root planing during pregnancy is associated with a reduction in the preterm birth rate.
Design: Systematic review and meta-analysis of randomised controlled trials.
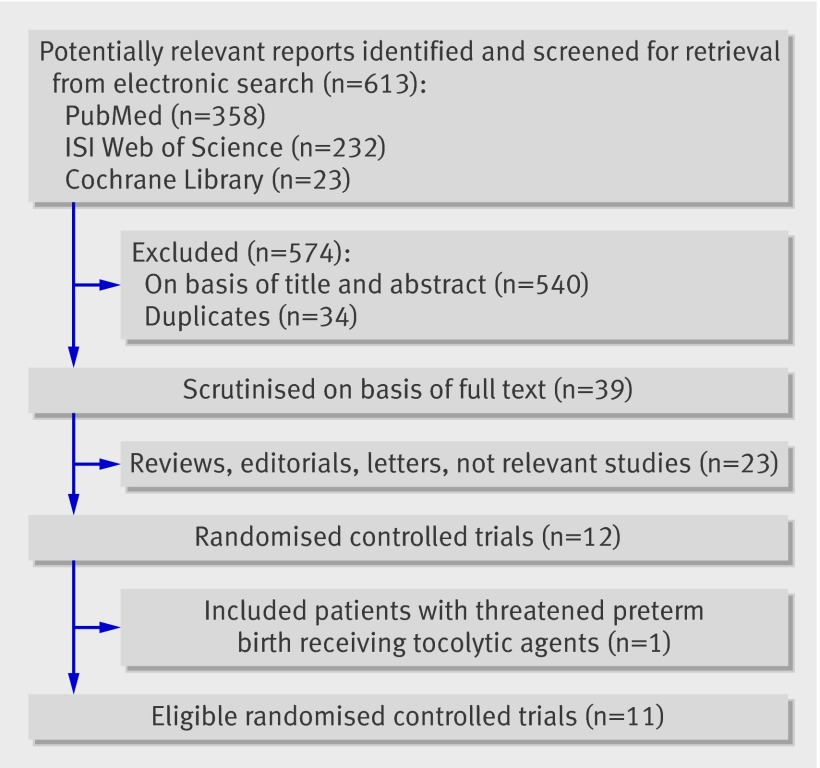
Data sources: Cochrane Central Trials Registry, ISI Web of Science, Medline, and reference lists of relevant studies to July 2010; hand searches in key journals.
Study selection: Randomised controlled trials including pregnant women with documented periodontal disease randomised to either treatment with scaling and root planing or no treatment.
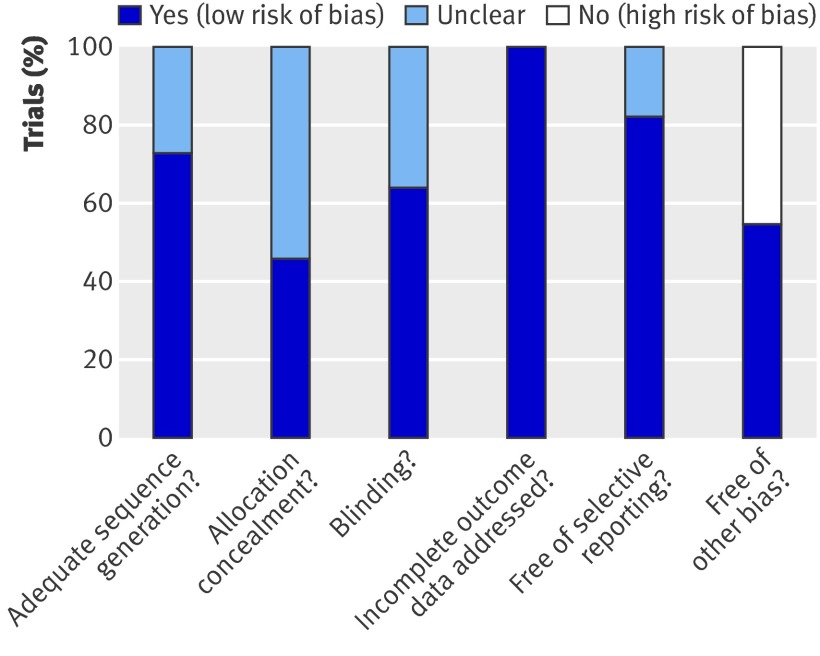
Data extraction: Data were extracted by two independent investigators, and a consensus was reached with the involvement a third. Methodological quality of the studies was assessed with the Cochrane's risk of bias tool, and trials were considered either high or low quality. The primary outcome was preterm birth (<37 weeks). Secondary outcomes were low birthweight infants (<2500 g), spontaneous abortions/stillbirths, and overall adverse pregnancy outcome (preterm birth <37 weeks and spontaneous abortions/stillbirths).
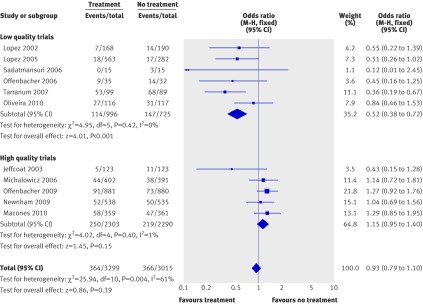
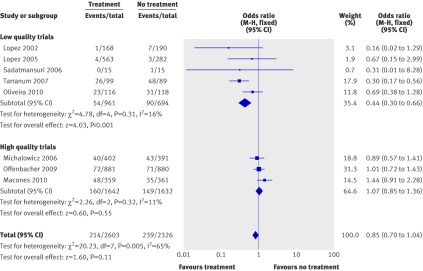
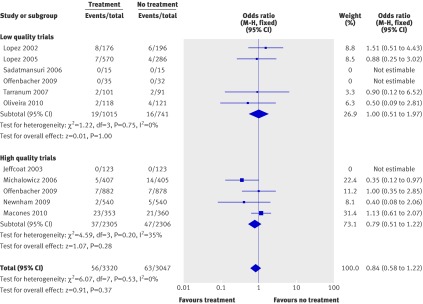
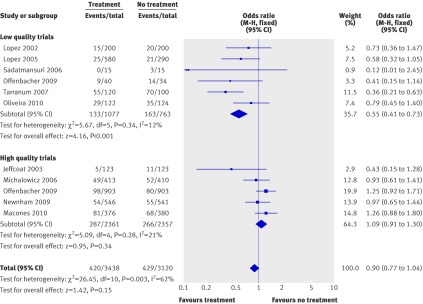
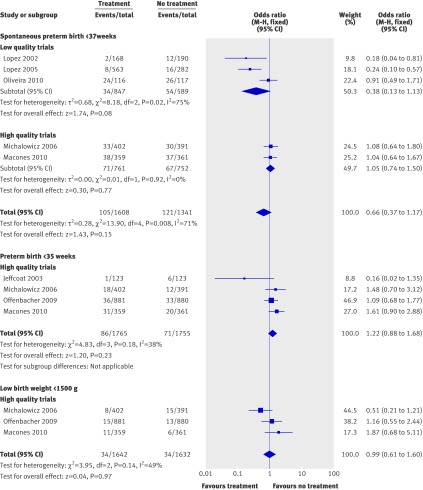
Results: 11 trials (with 6558 women) were included. Five trials were considered to be of high methodological quality (low risk of bias), whereas the rest were low quality (high or unclear risk of bias). Results among low and high quality trials were consistently diverse; low quality trials supported a beneficial effect of treatment, and high quality trials provided clear evidence that no such effect exists. Among high quality studies, treatment had no significant effect on the overall rate of preterm birth (odds ratio 1.15, 95% confidence interval 0.95 to 1.40; P=0.15). Furthermore, treatment did not reduce the rate of low birthweight infants (odds ratio 1.07, 0.85 to 1.36; P=0.55), spontaneous abortions/stillbirths (0.79, 0.51 to 1.22; P=0.28), or overall adverse pregnancy outcome (preterm births <37 weeks and spontaneous abortions/stillbirths) (1.09, 0.91 to 1.30; P=0.34).
Conclusion: Treatment of periodontal disease with scaling and root planing cannot be considered to be an efficient way of reducing the incidence of preterm birth. Women may be advised to have periodical dental examinations during pregnancy to test their dental status and may have treatment for periodontal disease. However, they should be told that such treatment during pregnancy is unlikely to reduce the risk of preterm birth or low birthweight infants.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Treatment of periodontal disease in pregnancy.BMJ. 2010 Dec 29;341:c7090. doi: 10.1136/bmj.c7090. BMJ. 2010. PMID: 21190967 No abstract available.
-
A meta-analysis of randomized controlled trials shows no evidence that periodontal treatment during pregnancy prevents adverse pregnancy outcomes.J Am Dent Assoc. 2011 Oct;142(10):1192-3. doi: 10.14219/jada.archive.2011.0089. J Am Dent Assoc. 2011. PMID: 21965493
-
Scaling and root debridement in pregnant women did not result in fewer preterm births.Evid Based Dent. 2011 Dec;12(4):112. doi: 10.1038/sj.ebd.6400827. Evid Based Dent. 2011. PMID: 22193655
-
CAT of the month. Periodontal therapy may not affect adverse pregnancy outcomes (UT CAT #560).Tex Dent J. 2012 May;129(5):456. Tex Dent J. 2012. PMID: 22779200 No abstract available.
References
-
- Macones GA, Parry S, Nelson DB, Strauss JF, Ludmir J, Cohen AW, et al. Treatment of localized periodontal disease in pregnancy does not reduce the occurrence of preterm birth: results from the Periodontal Infections and Prematurity Study (PIPS). Am J Obstet Gynecol 2010;202:147,e1-8. - PubMed
-
- Laine MA. Effect of pregnancy on periodontal and dental health. Acta Odontol Scand 2002;60:257-64. - PubMed
-
- Michalowicz BS, DiAngelis AJ, Novak MJ, Buchanan W, Papapanou PN, Mitchell DA, et al. Examining the safety of dental treatment in pregnant women. J Am Dent Assoc 2008;139:685-95. - PubMed
-
- Offenbacher S, Katz V, Fertik G, Collins J, Boyd D, Maynor G, et al. Periodontal infection as a possible risk factor for preterm low birth weight. J Periodontol 1996;67(suppl 10):1103-13. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical