

Pathological classification of intrahepatic cholangiocarcinoma based on a new concept
- PMID: 21191517
- PMCID: PMC3010511
- DOI: 10.4254/wjh.v2.i12.419
Pathological classification of intrahepatic cholangiocarcinoma based on a new concept
Abstract
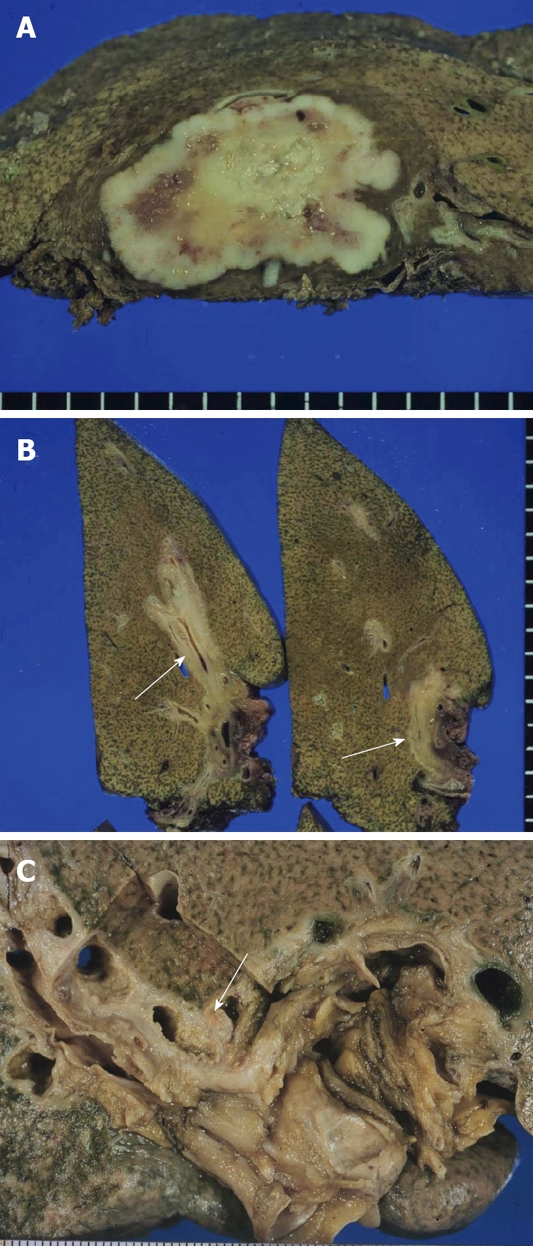
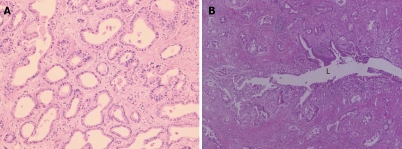
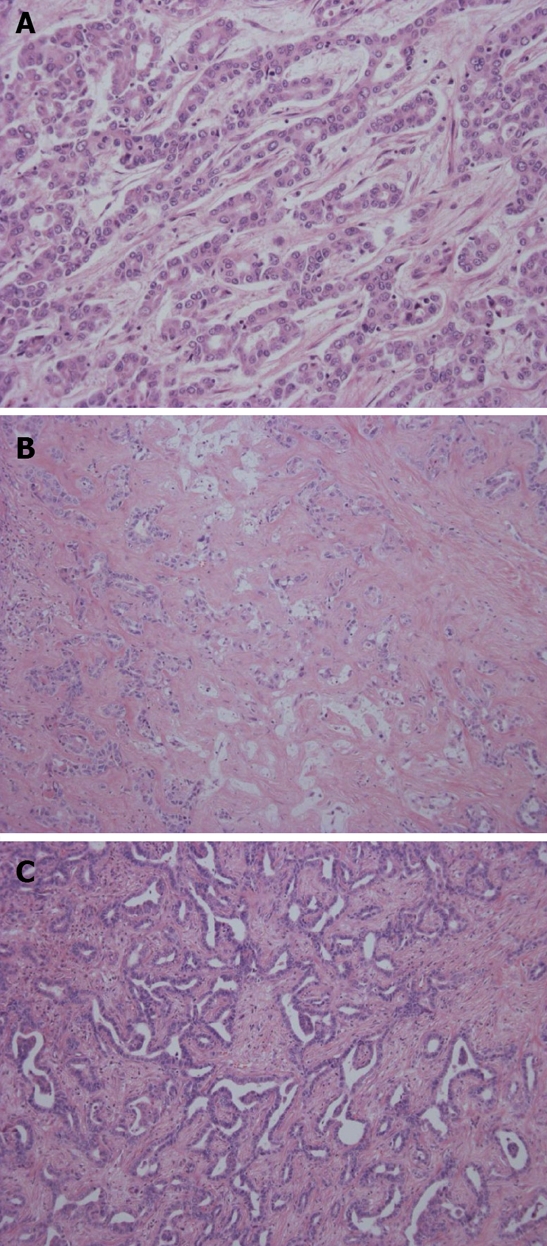
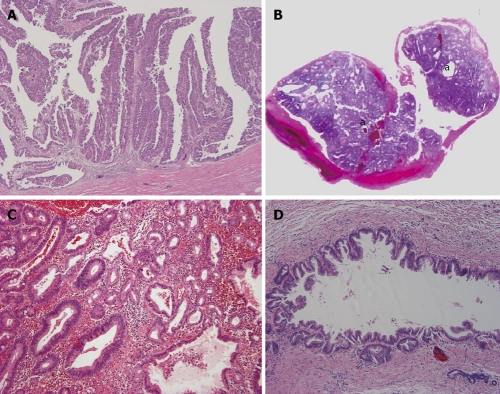
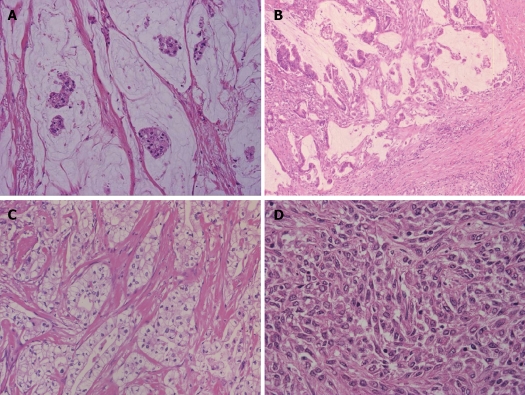
Intrahepatic cholangiocarcinoma (ICC) arises from the lining epithelium and peribiliary glands of the intrahepatic biliary tree and shows variable cholangiocytic differentiation. To date, ICC was largely classified into adenocarcinoma and rare variants. Herein, we propose to subclassify the former, based on recent progress in the study of ICC including the gross classification and hepatic progenitor/stem cells and on the pathological similarities between biliary and pancreatic neoplasms. That is, ICC is classifiable into the conventional (bile duct) type, the bile ductular type, the intraductal neoplasm type and rare variants. The conventional type is further divided into the small duct type (peripheral type) and large bile duct type (perihilar type). The former is a tubular or micropapillary adenocarcinoma while the latter involves the intrahepatic large bile duct. Bile ductular type resembles proliferated bile ductules and shows a replacing growth of the hepatic parenchyma. Hepatic progenitor cell or stem cell phenotypes such as neural cell adhesion molecule expression are frequently expressed in the bile ductular type. Intraductal type includes papillary and tubular neoplasms of the bile duct (IPNBs and ITNBs) and a superficial spreading type. IPNB and ITNB show a spectrum from a preneoplastic borderline lesion to carcinoma and may have pancreatic counterparts. At invasive sites, IPNB is associated with the conventional bile duct ICC and mucinous carcinoma. Biliary mucinous cystic neoplasm with ovarian-like stroma in its wall is different from IPNB, particularly IPNB showing cystic dilatation of the affected ducts. Rare variants of ICC include squamous/adenosquamous cell carcinoma, mucinous/signet ring cell carcinoma, clear cell type, undifferentiated type, neuroendocrine carcinoma and so on. This classification of ICC may open up a new field of research of ICC and contribute to the clinical approach to ICC.
Keywords: Adenocarcinoma; Bile duct; Bile ductule; Intraductal neoplasm; Intrahepatic cholangiocarcinoma.
Figures
References
-
- Nakanuma Y, Sripa B, Batanasapt V, Leong ASY, Ponchon T, Ishak KG. Intrahepatic cholangiocarcinoma. In: Pathology and Genetics., editor. Tumours of the Digestive System. World Health Organization of Tumours (Hamilton SR, Aaltonen LA, editors) IARC Press: Lyon; 2000. pp. 173–180.
-
- Nakanuma Y, Sasaki M, Ikeda H, Sato Y, Zen Y, Kosaka K, Harada K. Pathology of peripheral intrahepatic cholangiocarcinoma with reference to tumorigenesis. Hepatol Res. 2008;38:325–334. - PubMed
-
- Reddy SB, Patel T. Current approaches to the diagnosis and treatment of cholangiocarcinoma. Curr Gastroenterol Rep. 2006;8:30–37. - PubMed
-
- Zen Y, Fujii T, Itatsu K, Nakamura K, Minato H, Kasashima S, Kurumaya H, Katayanagi K, Kawashima A, Masuda S, et al. Biliary papillary tumors share pathological features with intraductal papillary mucinous neoplasm of the pancreas. Hepatology. 2006;44:1333–1343. - PubMed
LinkOut - more resources
Full Text Sources
