

Ergonovine stress echocardiography: Recent experience and safety in our centre
- PMID: 21191545
- PMCID: PMC3011139
- DOI: 10.4330/wjc.v2.i12.437
Ergonovine stress echocardiography: Recent experience and safety in our centre
Abstract
Aim: To study recent experience and safety of ergonovine stress echocardiography in our centre.
Methods: In this study we collected the clinical variables of patients referred since 2002 for ergonovine stress echocardiography, in addition to indications, the results of this test, complications, blood pressure and heart rate values during the test and the number and results of tests requested before this technique.
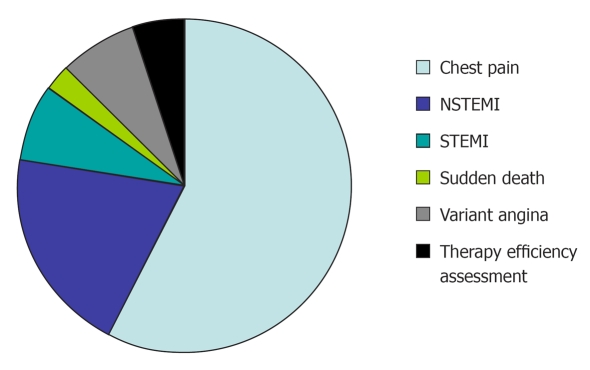
Results: We performed 40 tests in 38 patients, 2 tests were carried out to verify therapy efficacy. The prevalence of classic cardiovascular risk factors was low and the most frequent indication was chest pain (57.5%). Coronary angiography was performed in 32 patients, and showed normal coronary arteries in 27 patients and non-significant stenosis in 5 cases. In 16 patients, coronary angiography was carried out after a positive or inconclusive ischemia test. Another 6 patients had a normal stress test (5 exercise electrocardiography tests and 1 nuclear imaging test). Of the 40 ergonovine stress echocardiography tests, 6 were positive (4 in the right coronary artery territory and 2 in the circumflex coronary artery territory), all of them by echocardiographic criteria, and by electrocardiographic criteria in only 3 (50%). The presence of non-significant coronary artery stenosis was more frequent in patients with positive ergonovine stress echocardiography (50% vs 6%, P = 0.038), and were related to ischemic territory. During the maximum stress stage, there was a higher systolic (130.26 ± 19.17 mmHg vs 136.58 ± 27.27 mmHg, 95% CI: -12.77 to 0.14 mmHg, P = 0.055) and diastolic blood pressure (77.89 ± 13.49 mmHg vs 83.95 ± 15.73 mmHg, 95% CI: -10.41 to -1.69 mmHg, P = 0.008) than at the baseline stage, and the same was registered with heart rate (73 ± 10.96 beats/min vs 79.79 ± 11.72 beats/min, 95% CI: -9.46 to -4.11 beats/min, P < 0.01). Nevertheless, there were only 2 hypertensive reactions during the last stage, which did not force a premature end to the test, without sustained tachy or bradyarrhythmias, and the technique was well tolerated in 58% of cases. A unique complication (2.5%) of this test was a prolonged vasospasm with a slight increase in necrosis biomarkers, however, this was without repercussion.
Conclusion: Ergonovine stress echocardiography can be performed with safety, is well tolerated in the majority of cases, and is useful for determining the ischemia mechanism in selected cases.
Keywords: Coronary angiography; Ergonovine; Myocardial ischaemia; Stress echocardiography; Vasospasm.
Figures


References
-
- Maseri A, L'Abbate A, Baroldi G, Chierchia S, Marzilli M, Ballestra AM, Severi S, Parodi O, Biagini A, Distante A, et al. Coronary vasospasm as a possible cause of myocardial infarction. A conclusion derived from the study of "preinfarction" angina. N Engl J Med. 1978;299:1271–1277. - PubMed
-
- Waters DD, Szlachcic J, Miller D, Theroux P. Clinical characteristics of patients with variant angina complicated by myocardial infarction or death within 1 month. Am J Cardiol. 1982;49:658–664. - PubMed
-
- Fukai T, Koyanagi S, Takeshita A. Role of coronary vasospasm in the pathogenesis of myocardial infarction: study in patients with no significant coronary stenosis. Am Heart J. 1993;126:1305–1311. - PubMed
-
- Cheng TO. Provocative tests for coronary artery spasm. Am J Cardiol. 1999;84:497–498. - PubMed
-
- Schroeder JS. Provocative testing for coronary artery spasm. Cardiovasc Clin. 1985;15:83–96. - PubMed
LinkOut - more resources
Full Text Sources
