

Chemoembolization decreases drop-off risk of hepatocellular carcinoma patients on the liver transplant list
- PMID: 21191590
- PMCID: PMC4137764
- DOI: 10.1007/s00270-010-0077-7
Chemoembolization decreases drop-off risk of hepatocellular carcinoma patients on the liver transplant list
Abstract
Introduction: The drop-off risk for patients awaiting liver transplantation for hepatocellular carcinoma (HCC) is 22%. Transplant liver availability is expected to worsen, resulting in longer waiting times and increased drop-off rates. Our aim was to determine whether chemoembolization can decrease this risk.
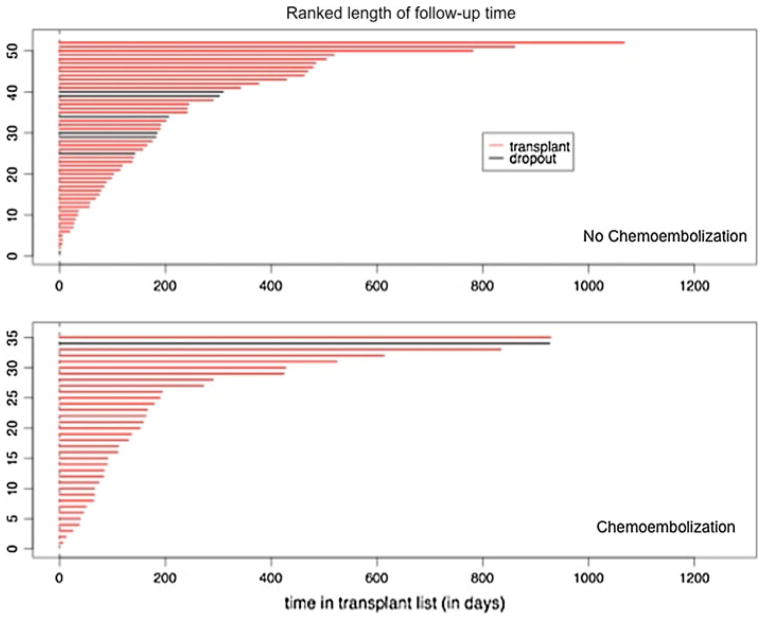
Patients and methods: Eighty-seven consecutive HCC patients listed for liver transplant (Milan criteria) underwent statistical comparability adjustments using the propensity score (Wilcoxon, Fisher's, and chi-square tests). Forty-three nonchemoembolization patients and 22 chemoembolization patients were comparable for Child-Pugh and Model for End-Stage Liver Disease scores, tumor size and number, alpha fetoprotein (AFP) levels, and cause of cirrhosis. We calculated the risk of dropping off the transplant list by assigning a transplant time to those who dropped off (equal probability with patients who were on the list longer than the patient in question). The significance level was obtained by calculating the simulation distribution of the difference compared with the permutations of chemoembolization versus nonchemoembolization assignment of the patients. Kaplan-Meier estimators (log-rank test) were used to determine survival rates.
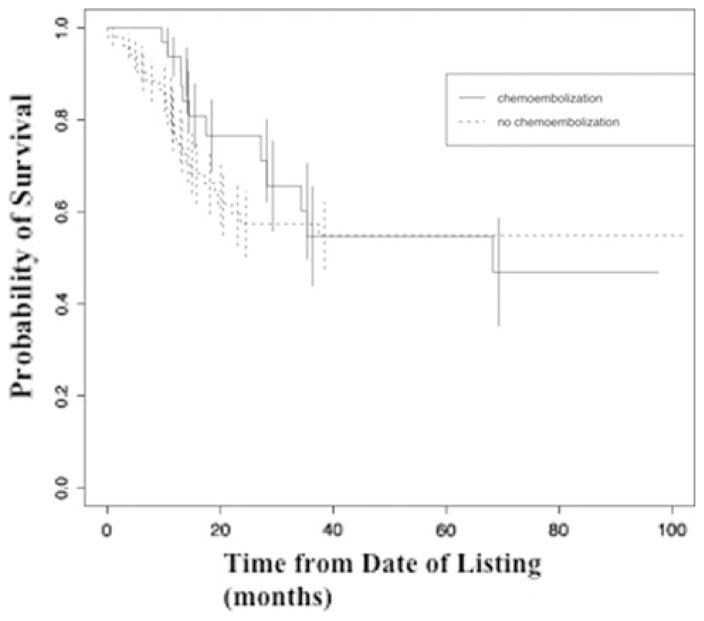
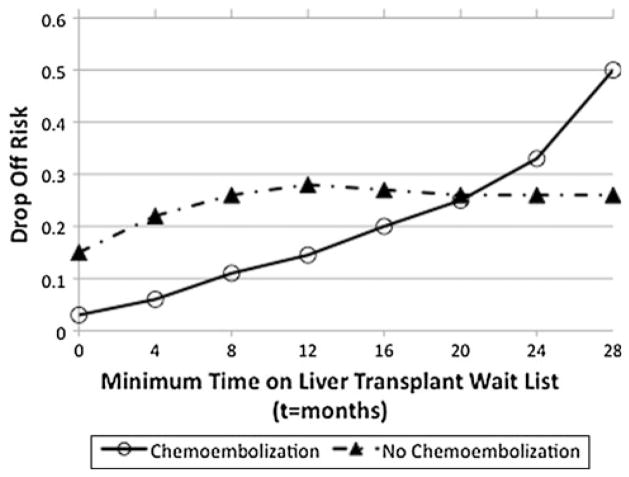
Results: Median follow-up was 187 ± 110 weeks (range 38 to 435, date of diagnosis). The chemoembolization group had an 80% drop-off risk decrease (15% nonchemoembolization versus 3% chemoembolization, p = 0.04). Although survival was better for the chemoembolization group, it did not reach statistical significance. Two-year survival for the nonchemoembolization and chemoembolization group was 57.3% ± 7.1% and 76.0% ± 7.9%, respectively (p = 0.078).
Conclusions: Chemoembolization appears to result in a significant decrease in the risk of dropping off liver transplant list for patients with HCC and results in a tendency toward longer survival.
Conflict of interest statement
Figures

References
-
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–699. - PubMed
-
- Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook A, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33:1394–1403. - PubMed
-
- Pelletier SJ, Fu S, Thyagarajan V, Romero-Marrero C, Batheja MJ, Punch JD, et al. An intention-to-treat analysis of liver transplantation for hepatocellular carcinoma using organ procurement transplant network data. Liver Transpl. 2009;15(8):859–868. - PubMed
-
- Stockland AH, Walser EM, Paz-Fumagalli R, McKinney JM, Mayrger GR. Preoperative chemoembolization in patients with hepatocellular carcinoma undergoing liver transplantation: influence of emergent versus elective procedures on patient survival and tumor recurrence rate. Cardiovasc Intervent Radiol. 2007;30:888–893. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
