

The effects of gatekeeping: a systematic review of the literature
- PMID: 21192758
- PMCID: PMC3347935
- DOI: 10.3109/02813432.2010.537015
The effects of gatekeeping: a systematic review of the literature
Abstract
Objective: To assess the effects of physician-centred gatekeeping on health, health care utilization, and costs by conducting a systematic review of the literature.
Methods: Systematic search in PubMed (MEDLINE and Pre-MEDLINE), EMBASE, and the Cochrane Library, from the databases' respective inception dates up to January 2010, using the search words "gatekeeping", "gatekeeper*", "first contact", and "self-referral". We included RCTs, CCTs, cohort studies, CBAs, and interrupted time-series. We included only studies in which the gatekeeper function was exercised by a physician and that reported health and patient-related outcomes including quality of life and satisfaction, quality of care, health care utilization, and/or economic outcomes (e.g. expenditures or efficiency). Selection was made independently by two reviewers and discrepancies were solved by consensus after discussion. Data on target population, intervention, additional interventions, study results, and methodological quality were extracted. Methodological quality was assessed independently by two reviewers following the previously defined criteria. Discrepancies were solved by consensus after discussion.
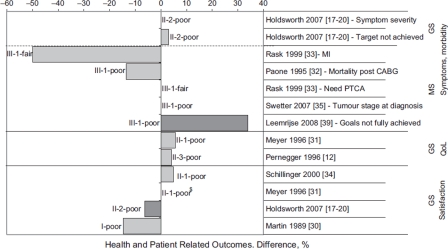
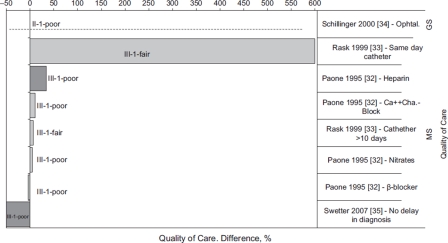
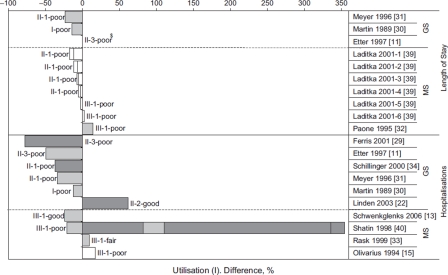
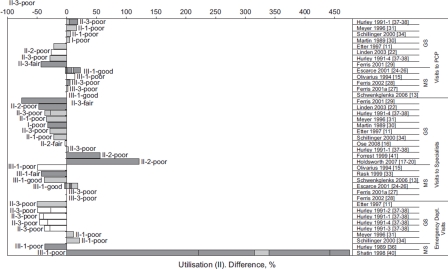
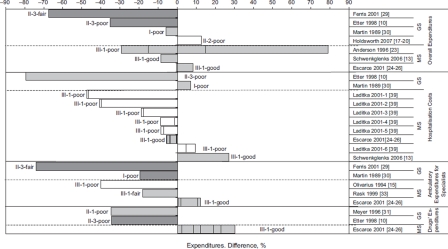
Results: This review includes 26 studies in 32 publications. The majority of studies (62%) reported data from the United States and in most gatekeeping was associated with lower utilization of health services (up to -78%) and lower expenditures (up to -80%). However, there was great variability in the magnitude and direction of the differences.
Conclusion: Overall, the evidence regarding the effects of gatekeeping is of limited quality. Many studies are available regarding the effects on health care utilisation and expenditures, whereas effects on health and patient-related outcomes have been studied only exceptionally and are inconclusive.
Figures
References
-
- Delnoij D, van Merode G, Paulus A, et al. Does general practitioner gatekeeping curb health care expenditure? J Health Serv Res Policy. 2000;5:22–6. - PubMed
-
- Franks P, Clancy CM, Nutting PA. Gatekeeping revisited, protecting patients from overtreatment. N Engl J Med. 1992;327:424–9. - PubMed
-
- Cooper PF, Simon KI, Vistnes J. A closer look at the managed care backlash. Med Care. 2006;44:I–4–I–11. - PubMed
-
- Fang H, Liu H, Rizzo JA. Has the use of physician gatekeepers declined among HMOs? Evidence from the United States. Int J Health Care Finance Econ. 2009;9:183–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources