

Reappraising the concept of massive transfusion in trauma
- PMID: 21192812
- PMCID: PMC3219977
- DOI: 10.1186/cc9394
Reappraising the concept of massive transfusion in trauma
Abstract
Introduction: The massive-transfusion concept was introduced to recognize the dilutional complications resulting from large volumes of packed red blood cells (PRBCs). Definitions of massive transfusion vary and lack supporting clinical evidence. Damage-control resuscitation regimens of modern trauma care are targeted to the early correction of acute traumatic coagulopathy. The aim of this study was to identify a clinically relevant definition of trauma massive transfusion based on clinical outcomes. We also examined whether the concept was useful in that early prediction of massive transfusion requirements could allow early activation of blood bank protocols.
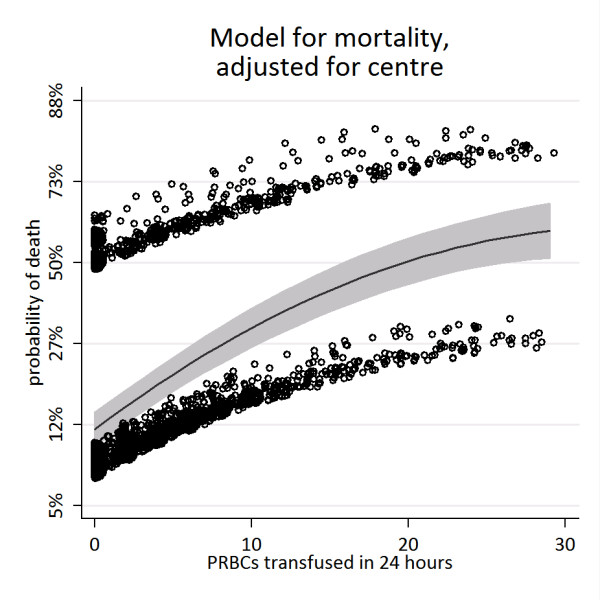
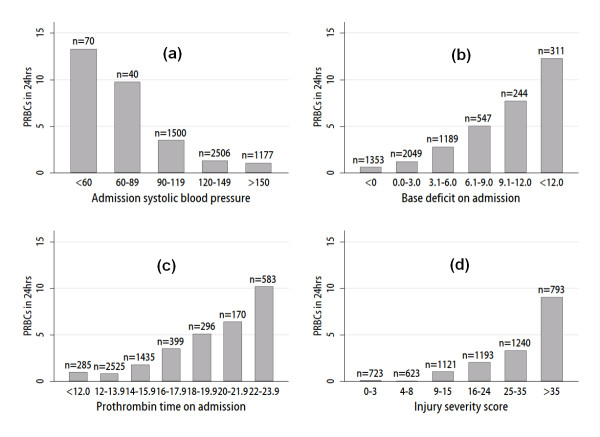
Methods: Datasets on trauma admissions over a 1 or 2-year period were obtained from the trauma registries of five large trauma research networks. A fractional polynomial was used to model the transfusion-associated probability of death. A logistic regression model for the prediction of massive transfusion, defined as 10 or more units of red cell transfusions, was developed.
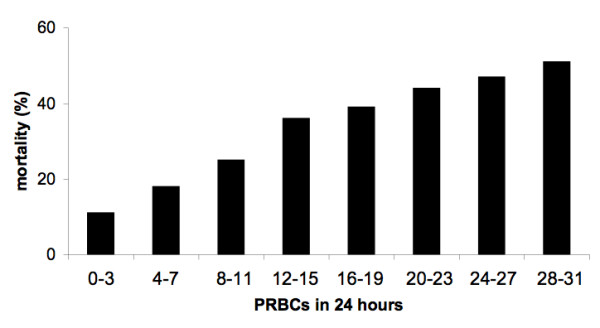
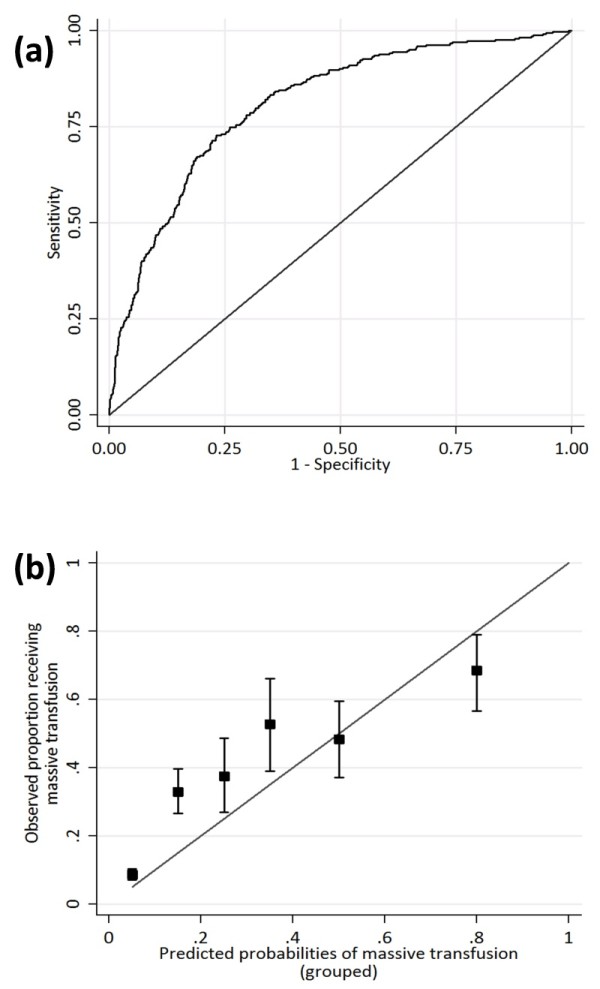
Results: In total, 5,693 patient records were available for analysis. Mortality increased as transfusion requirements increased, but the model indicated no threshold effect. Mortality was 9% in patients who received none to five PRBC units, 22% in patients receiving six to nine PRBC units, and 42% in patients receiving 10 or more units. A logistic model for prediction of massive transfusion was developed and validated at multiple sites but achieved only moderate performance. The area under the receiver operating characteristic curve was 0.81, with specificity of only 50% at a sensitivity of 90% for the prediction of 10 or more PRBC units. Performance varied widely at different trauma centers, with specificity varying from 48% to 91%.
Conclusions: No threshold for definition exists at which a massive transfusion specifically results in worse outcomes. Even with a large sample size across multiple trauma datasets, it was not possible to develop a transportable and clinically useful prediction model based on available admission parameters. Massive transfusion as a concept in trauma has limited utility, and emphasis should be placed on identifying patients with massive hemorrhage and acute traumatic coagulopathy.
Figures
Comment in
-
Resuscitation of the trauma patient: tell me a trigger for early haemostatic resuscitation please!Crit Care. 2011 Mar 1;15(2):126. doi: 10.1186/cc10014. Crit Care. 2011. PMID: 21371347 Free PMC article.
