

Metachronous colorectal cancer risk for mismatch repair gene mutation carriers: the advantage of more extensive colon surgery
- PMID: 21193451
- PMCID: PMC3848416
- DOI: 10.1136/gut.2010.228056
Metachronous colorectal cancer risk for mismatch repair gene mutation carriers: the advantage of more extensive colon surgery
Abstract
Background: Surgical management of colon cancer for patients with Lynch syndrome who carry a mismatch repair (MMR) gene mutation is controversial. The decision to remove more or less of the colon involves the consideration of a relatively high risk of metachronous colorectal cancer (CRC) with the impact of more extensive surgery.
Objective: To estimate and compare the risks of metachronous CRC for patients with Lynch syndrome undergoing either segmental or extensive (subtotal or total) resection for first colon cancer.
Design: Risk of metachronous CRC was estimated for 382 MMR gene mutation carriers (172 MLH1, 167 MSH2, 23 MSH6 and 20 PMS2) from the Colon Cancer Family Registry, who had surgery for their first colon cancer, using retrospective cohort analysis. Age-dependent cumulative risks of metachronous CRC were calculated using the Kaplan-Meier method. Risk factors for metachronous CRC were assessed by a Cox proportional hazards regression.
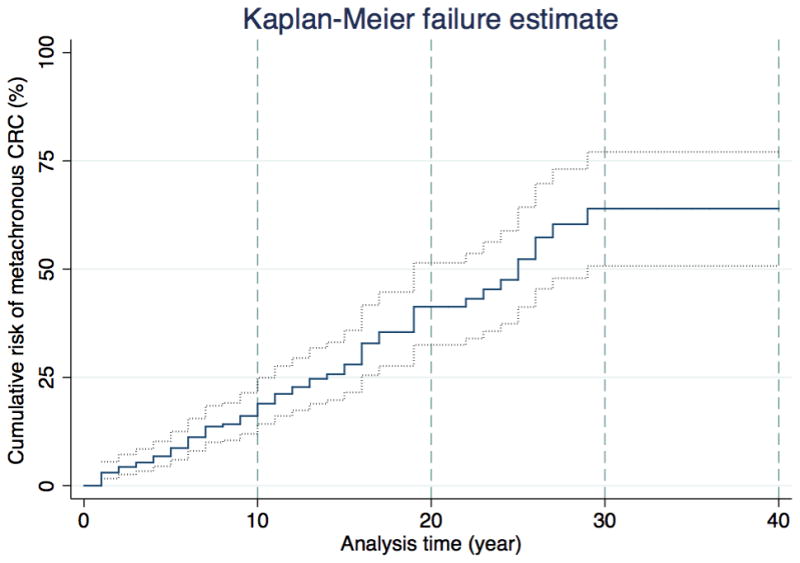
Results: None of 50 subjects who had extensive colectomy was diagnosed with metachronous CRC (incidence rate 0.0; 95% CI 0.0 to 7.2 per 1000 person-years). Of 332 subjects who had segmental resections, 74 (22%) were diagnosed with metachronous CRC (incidence rate 23.6; 95% CI 18.8 to 29.7 per 1000 person-years). For those who had segmental resections, incidence was statistically higher than for those who had extensive surgery (P <0.001). Cumulative risk of metachronous CRC was 16% (95% CI 10% to 25%) at 10 years, 41% (95% CI 30% to 52%) at 20 years and 62% (95% CI 50% to 77%) at 30 years after segmental colectomy. Risk of metachronous CRC reduced by 31% (95% CI 12% to 46%; p=0.002) for every 10 cm of bowel removed.
Conclusions: Patients with Lynch syndrome with first colon cancer treated with more extensive colonic resection have a lower risk of metachronous CRC than those receiving less extensive surgery. This finding will better inform decision-making about the extent of primary surgical resection.
Conflict of interest statement
The authors have no conflict of interest to declare with respect to this manuscript.
Figures
Comment in
-
Cumulative incidence of metachronous colorectal cancer risk for mismatch repair gene mutation carriers is overestimated.Gut. 2012 May;61(5):783; author reply 783-4. doi: 10.1136/gutjnl-2011-300997. Epub 2011 Aug 26. Gut. 2012. PMID: 21873468 No abstract available.
References
-
- Vasen HFA, Watson P, Mecklin JP, et al. New clinical criteria for hereditary nonpolyposis colorectal cancer (HNPCC, Lynch syndrome) proposed by the International Collaborative Group on HNPCC. Gastroenterology. 1999;116:1453–6. - PubMed
-
- Jenkins MA, Baglietto L, Dowty JG, et al. Cancer Risks For Mismatch Repair Gene Mutation Carriers: A Population-Based Early Onset Case-Family Study. Clinical gastroenterology and hepatology. 2006;4:489–98. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous