

Postrelapse survival in childhood acute lymphoblastic leukemia is independent of initial treatment intensity: a report from the Children's Oncology Group
- PMID: 21193696
- PMCID: PMC3062307
- DOI: 10.1182/blood-2010-07-294678
Postrelapse survival in childhood acute lymphoblastic leukemia is independent of initial treatment intensity: a report from the Children's Oncology Group
Abstract
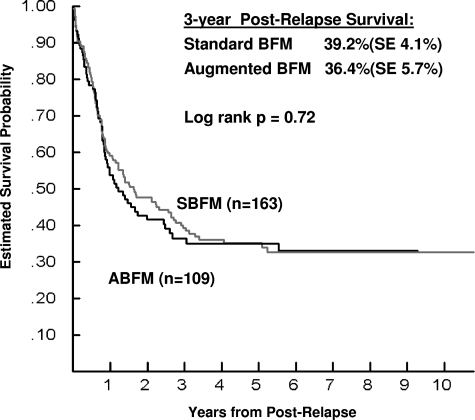
While intensification of therapy has improved event-free survival (EFS) and survival in newly diagnosed children with acute lymphoblastic leukemia (ALL), postrelapse outcomes remain poor. It might be expected that patients relapsing after inferior initial therapy would have a higher retrieval rate than after superior therapy. In the Children's Oncology Group Study CCG-1961, significantly superior EFS and survival were achieved with an augmented (stronger) versus standard intensity regimen of postinduction intensification (PII) for children with newly diagnosed high-risk ALL and rapid day 7 marrow response (EFS/survival 81.2%/88.7% vs 71.7%/83.4%, respectively). This provided an opportunity to evaluate postrelapse survival (PRS) in 272 relapsed patients who had received randomly allocated initial treatment with augmented or standard intensity PII. As expected, PRS was worse for early versus late relapse, marrow versus extramedullary site, adolescent versus younger age and T versus B lineage. However, no difference in 3-year PRS was detected for having received augmented versus standard intensity PII (36.4% ± 5.7% vs 39.2% ± 4.1%; log rank P = .72). Similar findings were noted within subanalyses by timing and site of relapse, age, and immunophenotype. These findings provide insight into mechanisms of relapse in ALL, and are consistent with emergence of a resistant subclone that has acquired spontaneous mutations largely independent of initial therapy. This study is registered at www.clinicaltrials.gov as NCT00002812.
Figures
References
-
- US Cancer Statistics Working Group. United States Cancer Statistics: 1999-2005 Incidence and Mortality Web-based Report. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; 2009. [Accessed May 28, 2010]. Available at http://www.cdc.gov/uscs.
-
- Trigg ME, Sather HN, Reaman GH, et al. Ten-year survival of children with acute lymphoblastic leukemia: a report from the Children's OncologyGroup. Leuk Lymphoma. 2008;49(6):1142–1154. - PubMed
-
- Conter V, Aricò M, Basso G, et al. Long-term results of the Italian Association of Pediatric Hematology and Oncology (AIEOP) studies 82, 87, 88, 91 and 95 for childhood acute lymphoblastic leukemia. Leukemia. 2010;24(2):255–264. - PubMed
-
- Möricke A, Zimmermann M, Reiter A, et al. Long-term results of five consecutive trials in childhood acute lymphoblastic leukemia performed by the ALL-BFM study group from 1981-2000. Leukemia. 2010;24(2):265–284. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
