

High-risk pediatric acute lymphoblastic leukemia: to transplant or not to transplant?
- PMID: 21195303
- PMCID: PMC3053056
- DOI: 10.1016/j.bbmt.2010.10.005
High-risk pediatric acute lymphoblastic leukemia: to transplant or not to transplant?
Abstract
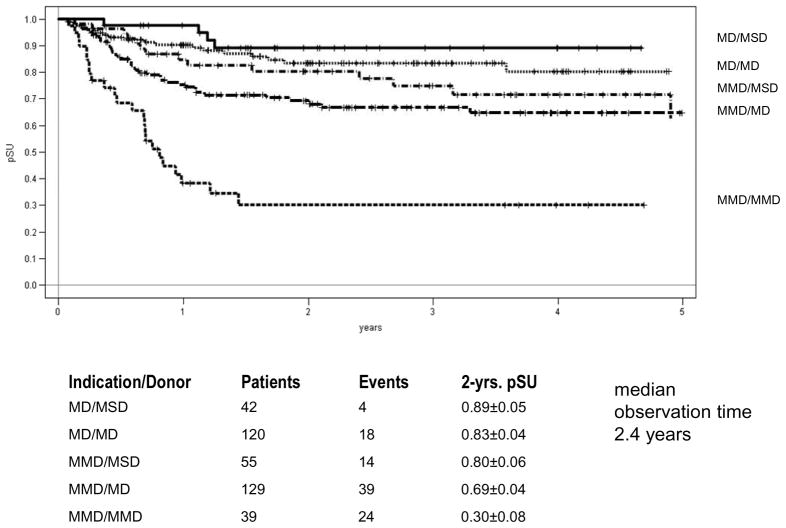
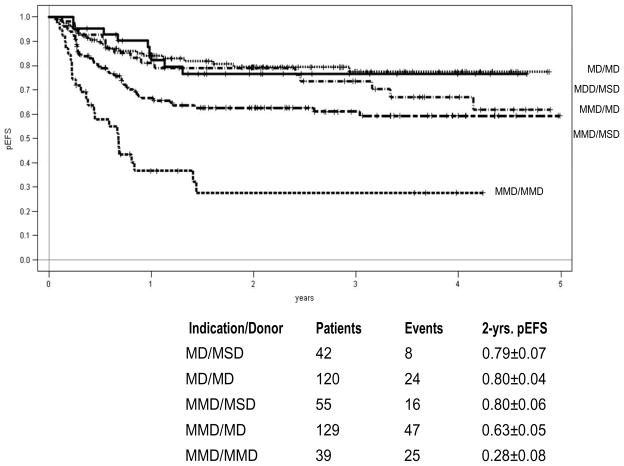
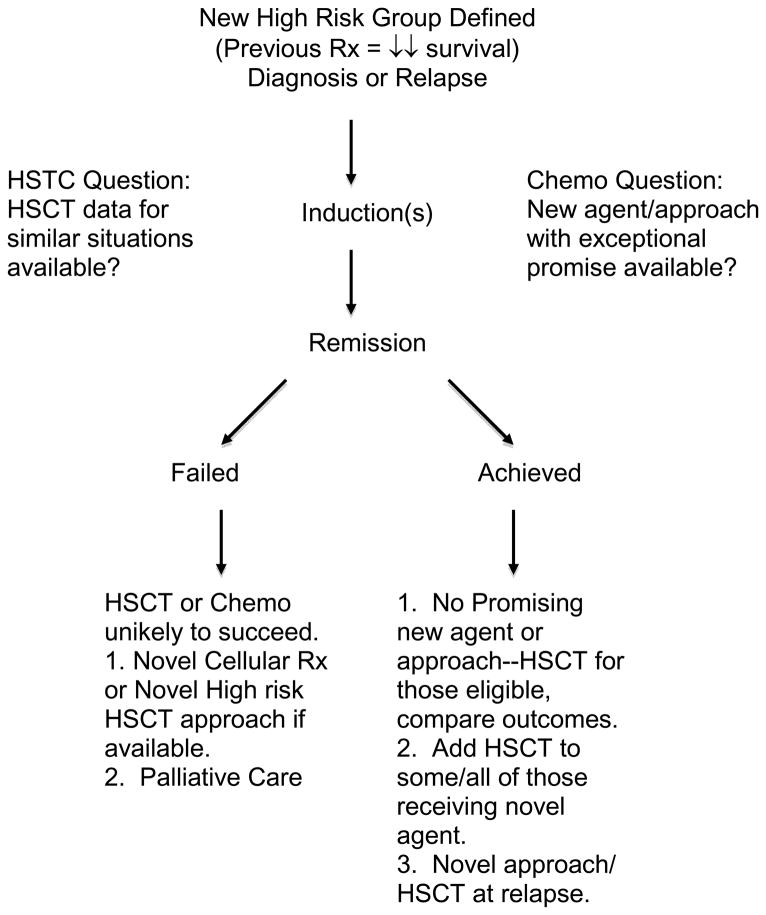
Because survival with both chemotherapy and allogeneic hematopoietic stem cell transplantation (HSCT) approaches to high-risk pediatric acute lymphoblastic leukemia (ALL) generally improves through the years, regular comparisons of outcomes with either approach for a given indication are needed to decide when HSCT is indicated. Improvements in risk classification are allowing clinicians to identify patients at high risk for relapse early in their course of therapy. Whether patients defined as high risk by new methods will benefit from HSCT requires careful testing. Standardization and improvement of transplant approaches has led to equivalent survival outcomes with matched sibling and well-matched unrelated donors; however, survival using mismatched and haploidentical donors is generally worse. Trials comparing chemotherapy and HSCT must obtain sufficient data about therapy and stratify the analysis to assess the outcomes of best-chemotherapy with best-HSCT approaches.
Copyright © 2011 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Moricke A, Zimmermann M, Reiter A, et al. Long-term results of five consecutive trials in childhood acute lymphoblastic leukemia performed by the ALL-BFM study group from 1981 to 2000. Leukemia. 2010;24:265–284. - PubMed
-
- Pulsipher MA, Bader P, Klingebiel T, Cooper LJ. Allogeneic transplantation for pediatric acute lymphoblastic leukemia: the emerging role of peritransplantation minimal residual disease/chimerism monitoring and novel chemotherapeutic, molecular, and immune approaches aimed at preventing relapse. Biol Blood Marrow Transplant. 2008;15:62–71. - PubMed
-
- Tallen G, Ratei R, Mann G, et al. Long-term outcome in children with relapsed acute lymphoblastic leukemia after time-point and site-of-relapse stratification and intensified short-course multidrug chemotherapy: results of trial ALL-REZ BFM 90. J Clin Oncol. 2010;28:2339–2347. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
