

Non-invasive predictors of esophageal varices
- PMID: 21196656
- PMCID: PMC3099085
- DOI: 10.4103/1319-3767.74470
Non-invasive predictors of esophageal varices
Abstract
Background/aim: Current guidelines recommend screening cirrhotic patients with an endoscopy to detect esophageal varices and to institute prophylactic measures in patients with large esophageal varices. In this study, we aimed at identifying non-endoscopic parameters that could predict the presence and grades of esophageal varices.
Patients and methods: In a prospective study, 229 newly diagnosed patients with liver cirrhosis, without a history of variceal bleeding, were included. Demographic, clinical, biochemical and ultrasonographic parameters were recorded. Esophageal varices were classified as small and large, at endoscopy. Univariate analysis and multivariate logistic regression analysis were done to identify independent predictors for the presence and grades of varices.
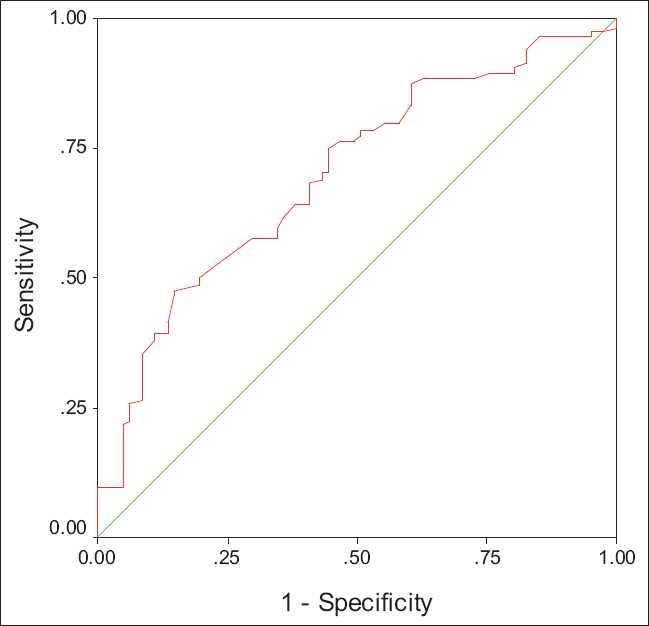
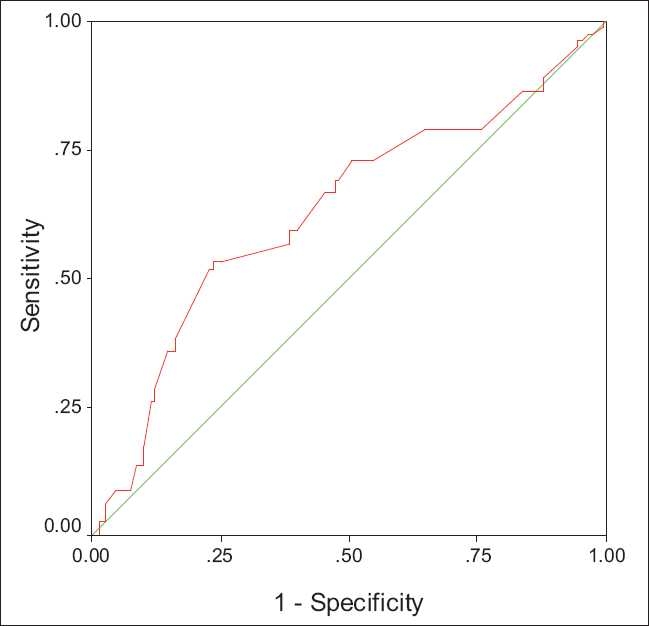
Results: Of the 229 patients (141 males; median age 42 years; range 17-73 years) with liver cirrhosis, 97 (42.3%) had small and 81 (35.4%) had large varices. On multivariate analysis, low platelet count (Odd's Ratio [OR], 4.3; 95% confidence interval [CI], 1.2-14.9), Child Pugh class B/C (OR, 3.3; 95% CI, 1.8-6.3), spleen diameter (OR, 4.3; 95% CI, 1.6-11.9) and portal vein diameter (OR, 2.4; 95% CI, 1.1-5.3) were independent predictors for the presence of varices. Likewise, for the presence of large esophageal varices, low platelet count (OR, 2.7; 95% CI, 1.4-5.2), Child Pugh class B/C (OR, 3.8; 95% CI, 2.3-6.5) and spleen diameter (OR, 3.1; 95% CI, 1.6-6.0) were the independent risk factors.
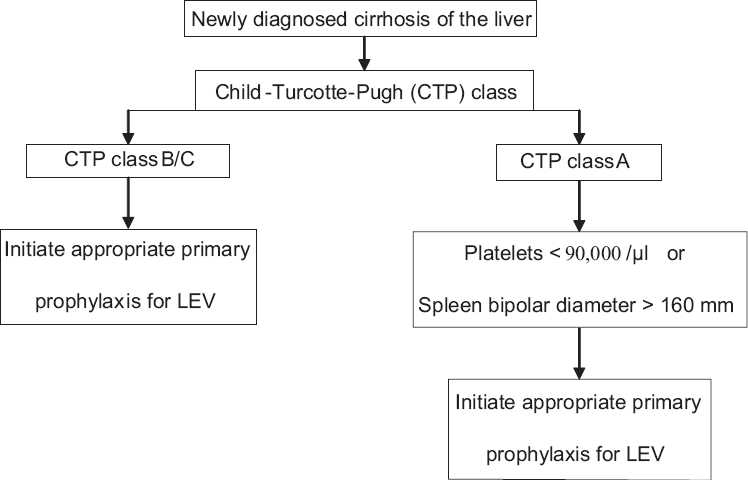
Conclusion: The presence and higher grades of varices can be predicted by a low platelet count, Child-Pugh class B/C and spleen diameter. These may be considered as non-endoscopic predictors for the diagnosis and management of large grade varices.
Conflict of interest statement
Figures
Comment in
-
Non-invasive prediction of esophageal varices: is it possible?Saudi J Gastroenterol. 2011 Jan-Feb;17(1):1-3. doi: 10.4103/1319-3767.74426. Saudi J Gastroenterol. 2011. PMID: 21196644 Free PMC article. No abstract available.
References
-
- Pagliaro L, D’Amico G, Pasta L, Politi F, Vizzini G, Traina M, et al. Portal hypertension in cirrhosis: Natural history. In: Bosch J, Groszmann RJ, editors. Portal Hypertension. Pathophysiology and Treatment. Oxford: Blackwell Scientific; 1994. pp. 72–92.
-
- Groszmann RJ, Garcia-Tsao G, Bosch J, Grace ND, Burroughs AK, Planas R, et al. Beta-blockers to prevent gastroesophageal varices in patients with cirrhosis. N Engl J Med. 2005;353:2254–61. - PubMed
-
- Merli M, Nicolini G, Angeloni S, Rinaldi V, De Santis A, Merkel C, et al. Incidence and natural history of small esophageal varices in cirrhotic patients. J Hepatol. 2003;38:266–72. - PubMed
-
- The North Italian Endoscopic Club for the Study and Treatment of Esophageal Varices. Prediction of the first variceal hemorrhage in patients with cirrhosis of the liver and esophageal varices. N Engl J Med. 1988;319:983–9. - PubMed
-
- Armonis A, Patch D, Burroughs AK. Hepatic venous pressure measurement: An old test as new prognostic marker in cirrhosis? Hepatology. 1997;25:245, 8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical