

doi: 10.4103/0972-9941.72367.
Single-incision laparoscopic cholecystectomy: How I do it?
Affiliations
- PMID: 21197237
- PMCID: PMC3002000
- DOI: 10.4103/0972-9941.72367
Item in Clipboard
Single-incision laparoscopic cholecystectomy: How I do it?
J Minim Access Surg.
2011 Jan.
Abstract
Single-incision laparoscopic cholecystectomy (SILC) is a relatively new technique that is being increasingly used by surgeons around the world. Unlike the multi-port cholecystectomy, a standardised technique and detailed description of the operative steps of SILC is lacking in the literature. This article provides a stepwise account of the technique of SILC aimed at surgeons wishing to learn the procedure. A brief review of the current literature on SILC follows.
Keywords: Cholecystectomy; Single-incision laparoscopic surgery; laparoscopy; single-port access surgery.
Conflict of interest statement
Figures

Long laparoscope (arrow) allows freedom of movement for operative instrument.

Positioning of the patient and the equipment (S = position of the surgeon, A = position of the assistant/camera person).

Two ports (10 and 5 mm) in the umbilical incision.
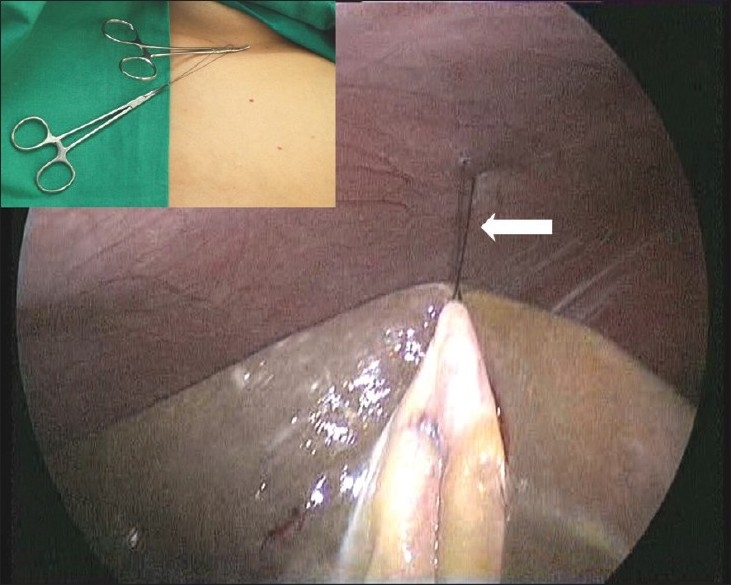
Cephalad elevation of the gallbladder via a fundal traction suture (arrow). Inset shows the traction suture held with hemostats.

Suspension of the gallbladder with a loop suture on the Hartmann’s pouch. Epigastric = suture entering from the epigastrium. Lateral = suture exiting from lateral abdominal wall.
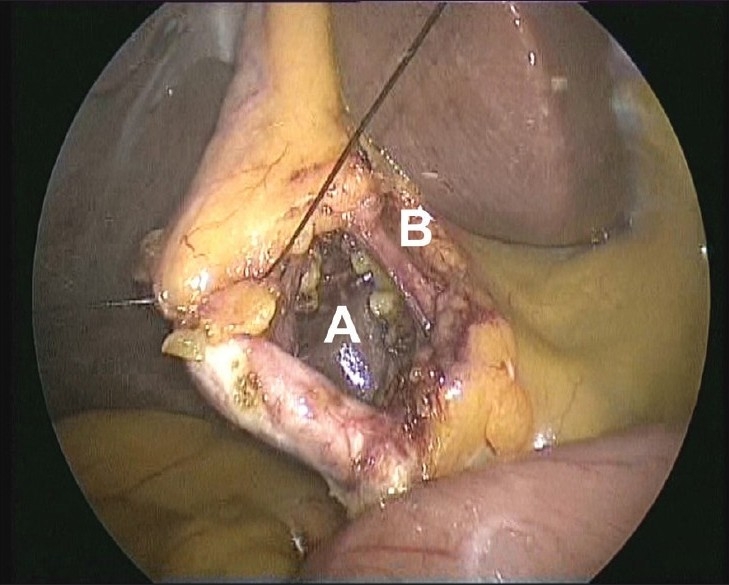
Critical view showing the window between the cystic duct and artery (A) and between the cystic artery and liver (B).
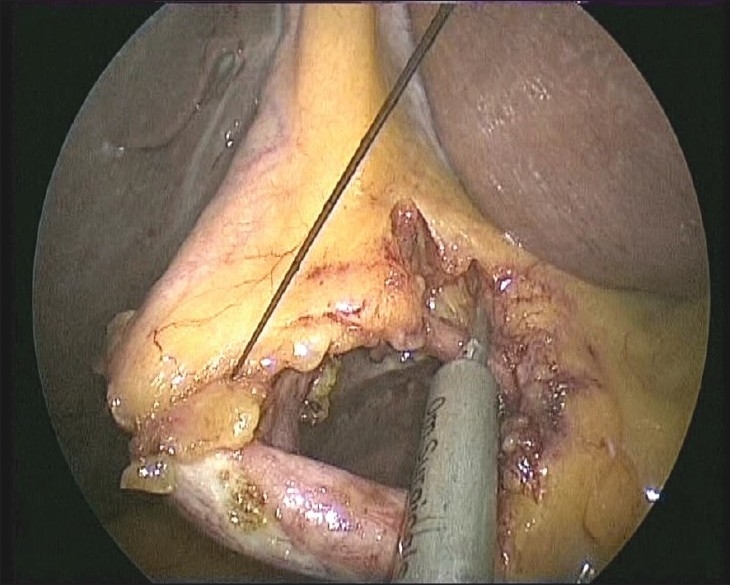
Cystic artery being clipped with a reusable 5-mm clip applicator.

Cystic duct being ligated using an extracorporeal knot (arrow).

Stones milked out from a partly opened cystic duct.
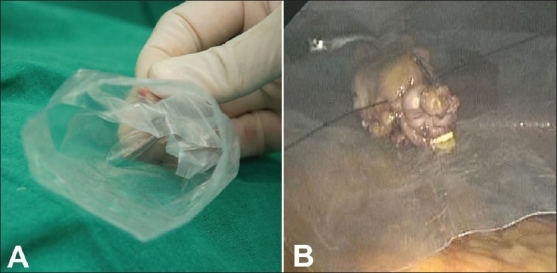
Everted plastic pouch stays open (A) and facilitates introduction of the gallbladder (B) for easy extraction.

Final appearance of transumbilical incision closed with subcuticular suture.
Similar articles
-
Prospective randomized comparison of single-incision laparoscopic cholecystectomy with new facilitating maneuver vs. conventional four-port laparoscopic cholecystectomy.Ulus Cerrahi Derg. 2016 Mar 1;32(1):23-9. doi: 10.5152/UCD.2015.3041. eCollection 2016. Ulus Cerrahi Derg. 2016. PMID: 26985165 Free PMC article.
-
Single incision laparoscopic cholecystectomy using the one-incision three-trocar technique with all straight instruments: how I do it?Front Med. 2011 Sep;5(3):283-7. doi: 10.1007/s11684-011-0151-9. Epub 2011 Oct 2. Front Med. 2011. PMID: 21964710 Review.
-
Single-incision laparoscopic cholecystectomy--can we afford that? Cost comparison of different surgical techniques.Pol Przegl Chir. 2014 Apr;86(4):177-80. doi: 10.2478/pjs-2014-0032. Pol Przegl Chir. 2014. PMID: 24988232
-
Single-incision laparoscopic cholecystectomy using glove port in comparison with standard laparoscopic cholecystectomy SILC using glove port.Surg Laparosc Endosc Percutan Tech. 2012 Feb;22(1):17-20. doi: 10.1097/SLE.0b013e318242e12a. Surg Laparosc Endosc Percutan Tech. 2012. PMID: 22318053
-
Single-Incision Laparoscopic Cholecystectomy: our experience and review of literature.G Chir. 2015 Nov-Dec;36(6):243-6. doi: 10.11138/gchir/2015.36.6.243. G Chir. 2015. PMID: 26888698 Free PMC article. Review.
Cited by
-
Cholecystomucoclasis: revaluation of safety and validity in aged populations.BMC Gastroenterol. 2012 Aug 21;12:113. doi: 10.1186/1471-230X-12-113. BMC Gastroenterol. 2012. PMID: 22909056 Free PMC article.
-
Two-port laparoscopic cholecystectomy with modified suture retraction of the fundus: A practical approach.J Minim Access Surg. 2013 Jul;9(3):122-5. doi: 10.4103/0972-9941.115372. J Minim Access Surg. 2013. PMID: 24019690 Free PMC article.
-
Prospective randomized comparison of single-incision laparoscopic cholecystectomy with new facilitating maneuver vs. conventional four-port laparoscopic cholecystectomy.Ulus Cerrahi Derg. 2016 Mar 1;32(1):23-9. doi: 10.5152/UCD.2015.3041. eCollection 2016. Ulus Cerrahi Derg. 2016. PMID: 26985165 Free PMC article.
-
The Transition from Open to Minimal Access Pediatric Surgery.J Indian Assoc Pediatr Surg. 2022 Mar-Apr;27(2):121-124. doi: 10.4103/jiaps.jiaps_227_21. Epub 2022 Mar 1. J Indian Assoc Pediatr Surg. 2022. PMID: 35937117 Free PMC article. No abstract available.
-
Single-incision laparoscopic surgery for biliary tract disease.World J Gastroenterol. 2016 Jan 14;22(2):736-47. doi: 10.3748/wjg.v22.i2.736. World J Gastroenterol. 2016. PMID: 26811621 Free PMC article. Review.
References
-
- Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I. One-wound laparoscopic cholecystectomy. Br J Surg. 1997;84:695. - PubMed
-
- Chow A, Purkayastha S, Aziz O, Paraskeva P. Single-incision laparoscopic surgery for cholecystectomy: An evolving technique. Surg Endosc. 2010;24:709–14. - PubMed
-
- Antoniou SA, Pointner R, Granderath FA. Single-incision laparoscopic cholecystectomy: A systematic review. Surg Endosc. 2010 - PubMed
LinkOut - more resources
Full Text Sources