

Acute pain management in children
- PMID: 21197314
- PMCID: PMC3004641
- DOI: 10.2147/jpr.s4554
Acute pain management in children
Abstract
The greatest advance in pediatric pain medicine is the recognition that untreated pain is a significant cause of morbidity and even mortality after surgical trauma. Accurate assessment of pain in different age groups and the effective treatment of postoperative pain is constantly being refined; with newer drugs being used alone or in combination with other drugs continues to be explored. Several advances in developmental neurobiology and pharmacology, knowledge of new analgesics and newer applications of old analgesics in the last two decades have helped the pediatric anesthesiologist in managing pain in children more efficiently. The latter include administering opioids via the skin and nasal mucosa and their addition into the neuraxial local anesthetics. Systemic opioids, nonsteroidal anti-inflammatory agents and regional analgesics alone or combined with additives are currently used to provide effective postoperative analgesia. These modalities are best utilized when combined as a multimodal approach to treat acute pain in the perioperative setting. The development of receptor specific drugs that can produce pain relief without the untoward side effects of respiratory depression will hasten the recovery and discharge of children after surgery. This review focuses on the overview of acute pain management in children, with an emphasis on pharmacological and regional anesthesia in achieving this goal.
Keywords: epidural additives; pain medication in children; pca and pcea in children; pediatric pain treatment; pediatric regional anesthesia.
Figures
References
-
- Malviya S, Polaner DM, Berde C. Acute pain. In: Cote CJ, Lerman J, Todres ID, editors. A practice of anesthesia for infants and children. Philadelphia: Saunders Elsevier; 2009. pp. 939–978.
-
- Verghese ST, Hannallah RS. Postoperative Pain Management in Children. Anesthesiology Clinics N Am. 2005;23:163–184. - PubMed
-
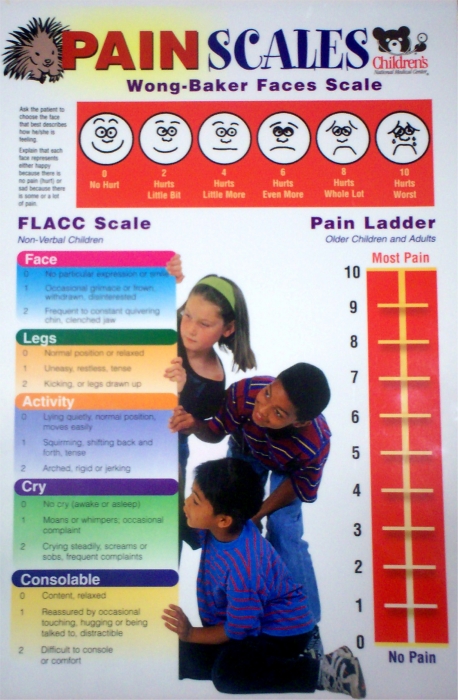
- O’Rouke D. The measurement of pain in infants, children, and adolescents: from policy to practice. Phys Ther. 2004;84:560–570. - PubMed
-
- Voepel-Lewis T, Merkel S, Tait AR, et al. The reliability and validity of the Face, Legs, Activity, Cry, Consolability observational tool as a measure of pain in children with cognitive impairment. Anesth Analg. 2002;95(5):1224–1229. - PubMed
-
- Birmingham PK, Tobin MJ, Fisher DM, et al. Initial and subsequent dosing of rectal acetaminophen in children- a 24-hour pharmacokinetic study of new dose recommendations. Anesthesiology. 2001;94:385–389. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
