

Cytomegalovirus latency promotes cardiac lymphoid neogenesis and accelerated allograft rejection in CMV naïve recipients
- PMID: 21199347
- PMCID: PMC3454525
- DOI: 10.1111/j.1600-6143.2010.03365.x
Cytomegalovirus latency promotes cardiac lymphoid neogenesis and accelerated allograft rejection in CMV naïve recipients
Abstract
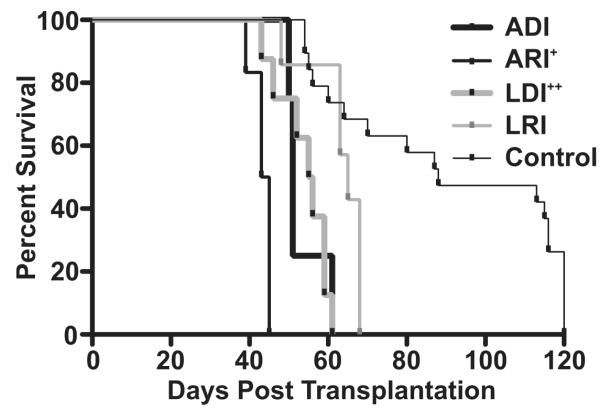
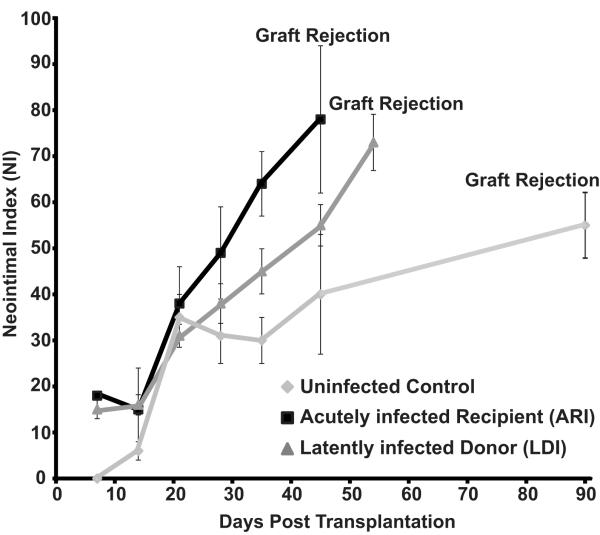
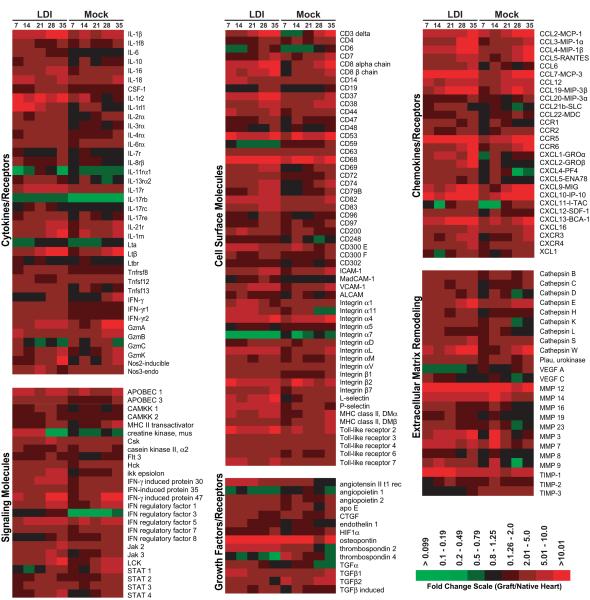
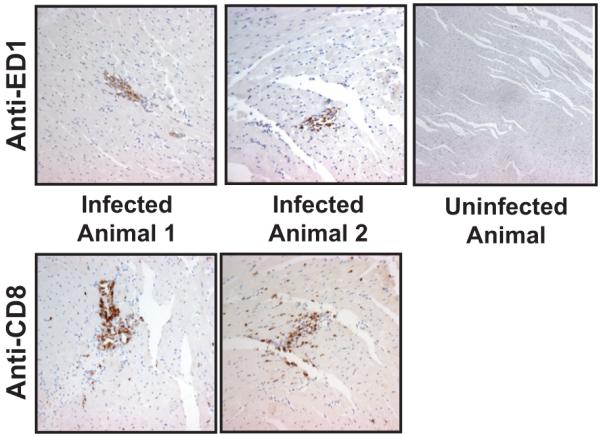
Human cytomegalovirus (HCMV) infection is associated with the acceleration of transplant vascular sclerosis (TVS) and chronic allograft rejection (CR). HCMV-negative recipients of latently HCMV infected donor grafts are at highest risk for developing CMV disease. Using a rat heart transplant CR model, we have previously shown that acute rat CMV (RCMV) infection following transplantation significantly accelerates both TVS and CR. Here, we report that RCMV-naïve recipients of heart allografts from latently RCMV-infected donors undergo acceleration of CR with similar kinetics as acutely infected recipients. In contrast to acutely infected recipients, treatment of recipients of latently infected donor hearts with ganciclovir did not prevent CR or TVS. We observed the formation of tertiary lymphoid structures (TLOs) containing macrophages and T cells in latently infected hearts prior to transplantation but not in uninfected rats. Moreover, pathway analysis of gene expression data from allografts from latently infected donors indicated an early and sustained production of TLO-associated genes compared to allografts from uninfected donors. We conclude that RCMV-induced TLO formation and alteration of donor tissue T cell profiles prior to transplantation in part mediate the ganciclovir-insensitive rejection of latently infected donor allografts transplanted into naïve recipients by providing a scaffold for immune activation.
©2010 The Authors Journal compilation©2010 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
-
- Almond PS, Matas A, Gillingham K, Dunn DL, Payne WD, Gores P, Gruessner R, Najarian JS. Risk factors for chronic rejection in renal allograft recipients. Transplant. 1993;55(4):752–6. discussion 756-7. - PubMed
-
- Isoniemi H, Nurminen M, Tikkanen MJ, von Willebrand E, Krogerus L, Ahonen J, Eklund B, Hockerstedt K, Salmela K, Hayry P. Risk factors predicting chronic rejection of renal allografts. Transplantation. 1994;57(1):68–72. - PubMed
-
- Fitzgerald JT, Gallay B, Taranto SE, McVicar JP, Troppmann C, Chen X, McIntosh MJ, Perez RV. Pretransplant recipient cytomegalovirus seropositivity and hemodialysis are associated with decreased renal allograft and patient survival. Transplantation. 2004;77(9):1405–11. - PubMed
-
- Grattan MT, Moreno-Cabral CE, Starnes VA, Oyer PE, Stinson EB, Shumway NE. Cytomegalovirus infection is associated with cardiac allograft rejection and atherosclerosis. JAMA. 1989;261(24):3561–6. - PubMed
