

Glioblastoma recurrence after cediranib therapy in patients: lack of "rebound" revascularization as mode of escape
- PMID: 21199795
- PMCID: PMC3074948
- DOI: 10.1158/0008-5472.CAN-10-2602
Glioblastoma recurrence after cediranib therapy in patients: lack of "rebound" revascularization as mode of escape
Erratum in
- Cancer Res. 2011 Mar 15;71(6):2405
Abstract
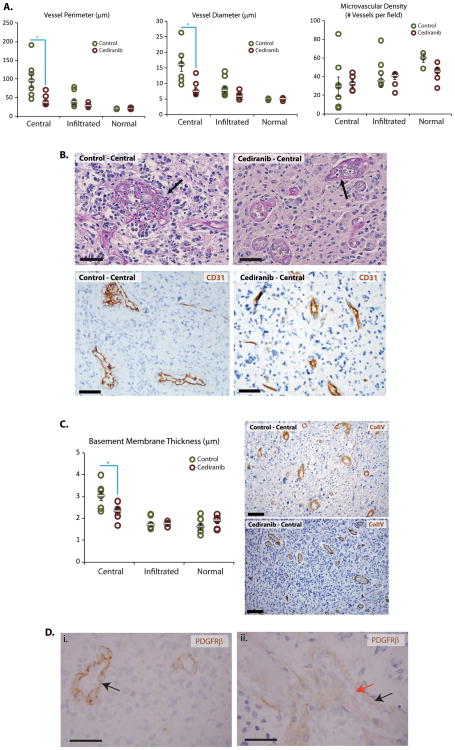
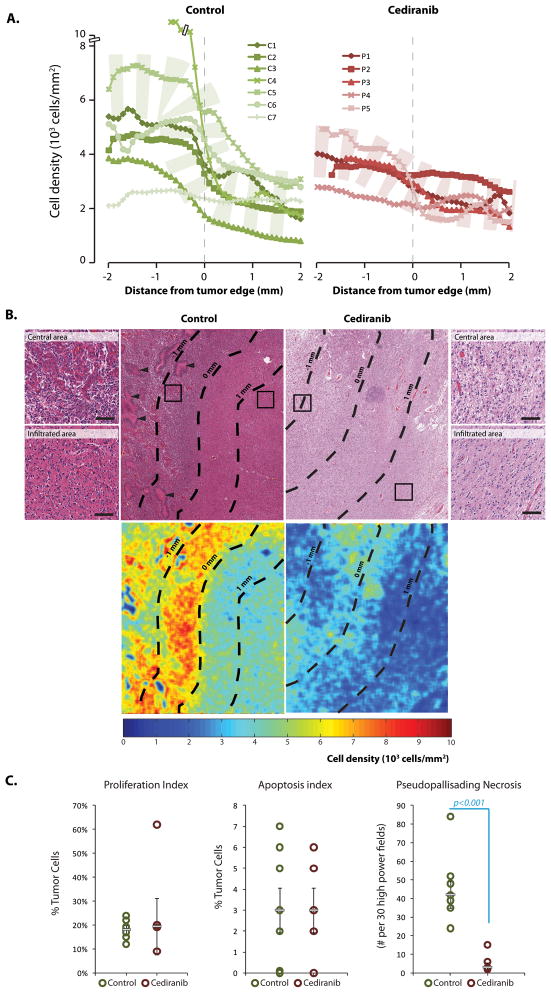
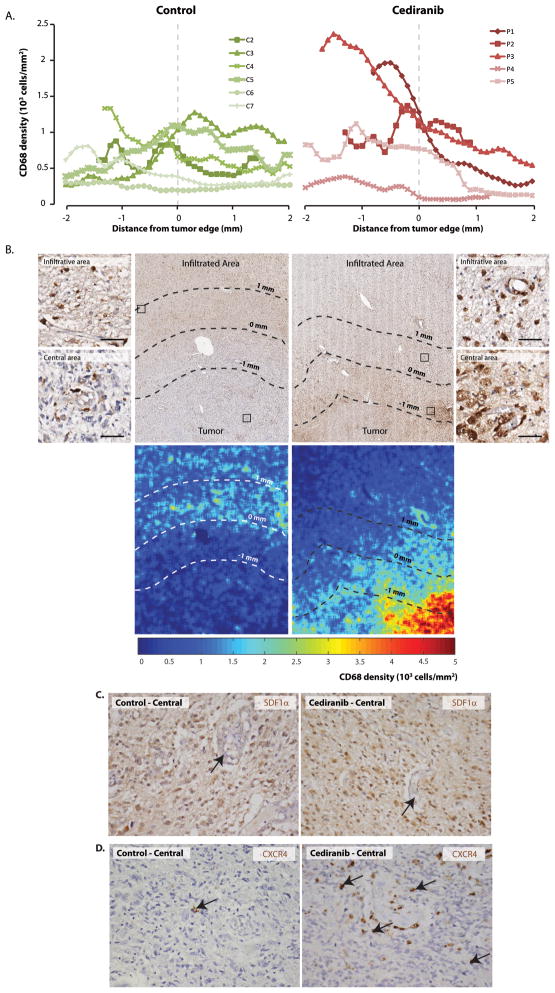
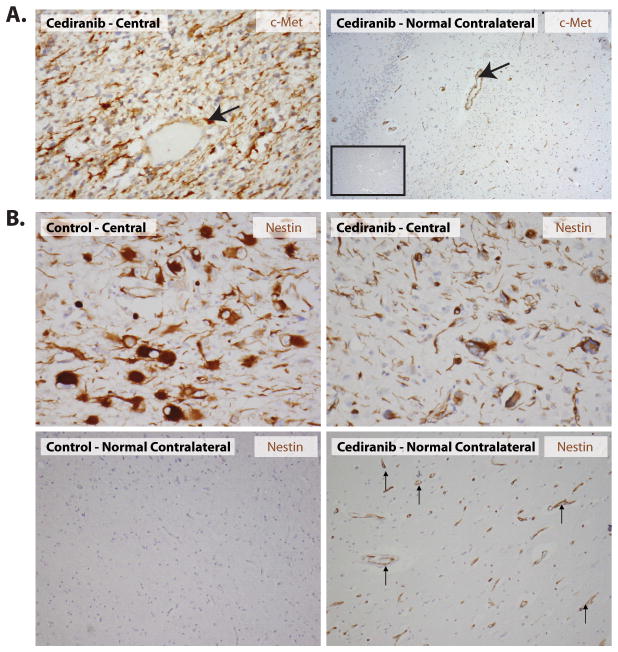
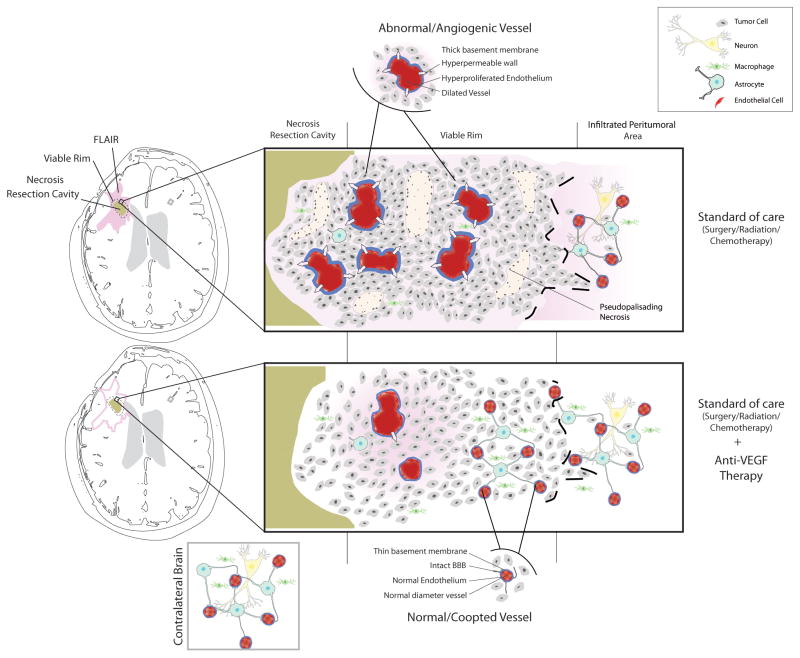
Recurrent glioblastomas (rGBM) invariably relapse after initial response to anti-VEGF therapy. There are 2 prevailing hypotheses on how these tumors escape antiangiogenic therapy: switch to VEGF-independent angiogenic pathways and vessel co-option. However, direct evidence in rGBM patients is lacking. Thus, we compared molecular, cellular, and vascular parameters in autopsy tissues from 5 rGBM patients who had been treated with the pan-VEGF receptor tyrosine kinase inhibitor cediranib versus 7 patients who received no therapy or chemoradiation but no antiangiogenic agents. After cediranib treatment, endothelial proliferation and glomeruloid vessels were decreased, and vessel diameters and perimeters were reduced to levels comparable to the unaffected contralateral brain hemisphere. In addition, tumor endothelial cells expressed molecular markers specific to the blood-brain barrier, indicative of a lack of revascularization despite the discontinuation of therapy. Surprisingly, in cediranib-treated GBM, cellular density in the central area of the tumor was lower than in control cases and gradually decreased toward the infiltrating edge, indicative of a change in growth pattern of rGBMs after cediranib treatment, unlike that after chemoradiation. Finally, cediranib-treated GBMs showed high levels of PDGF-C (platelet-derived growth factor C) and c-Met expression and infiltration by myeloid cells, which may potentially contribute to resistance to anti-VEGF therapy. In summary, we show that rGBMs switch their growth pattern after anti-VEGF therapy--characterized by lower tumor cellularity in the central area, decreased pseudopalisading necrosis, and blood vessels with normal molecular expression and morphology--without a second wave of angiogenesis.
© 2011 AACR.
Figures
References
-
- Jain RK, di Tomaso E, Duda DG, Loeffler JS, Sorensen AG, Batchelor TT. Angiogenesis in brain tumours. Nature reviews. 2007;8(8):610–22. - PubMed
-
- Plate KH, Mennel HD. Vascular morphology and angiogenesis in glial tumors. Exp Toxicol Pathol. 1995;47(2–3):89–94. - PubMed
-
- Rampling R, Cruickshank G, Lewis A, Fitzsimmon S, Workman P. Direct measurment of PO2 distribution and bioreductive enzymes in human malignant brain tumors. Int J Radiat Oncol Biol Phys. 1994;29(3):427–31. - PubMed
-
- Valk PE, Mathis CA, Prados MD, Gilbert JC, Budinger TF. Hypoxia in human gliomas: demonstration by PET with fluorine-18-fluoromisonidazole. J Nucl Med. 1992;33(12):2133–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P41-RR014075/RR/NCRR NIH HHS/United States
- R21 CA117079/CA/NCI NIH HHS/United States
- R01-CA115767/CA/NCI NIH HHS/United States
- P01-CA80124/CA/NCI NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- P01 CA080124/CA/NCI NIH HHS/United States
- R01-CA129371/CA/NCI NIH HHS/United States
- K24-CA125440/CA/NCI NIH HHS/United States
- M01-RR-01066/RR/NCRR NIH HHS/United States
- R01 CA129371/CA/NCI NIH HHS/United States
- P41 RR014075/RR/NCRR NIH HHS/United States
- K24 CA125440/CA/NCI NIH HHS/United States
- R01 CA115767/CA/NCI NIH HHS/United States
- R21-CA117079/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
