

Influence of continuous venovenous hemofiltration and continuous venovenous hemodiafiltration on the disposition of doripenem
- PMID: 21199922
- PMCID: PMC3067072
- DOI: 10.1128/AAC.01063-10
Influence of continuous venovenous hemofiltration and continuous venovenous hemodiafiltration on the disposition of doripenem
Abstract
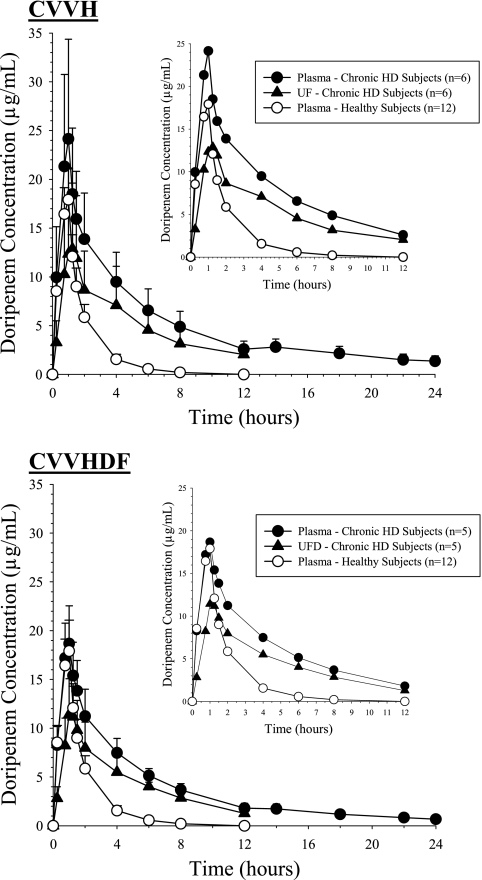
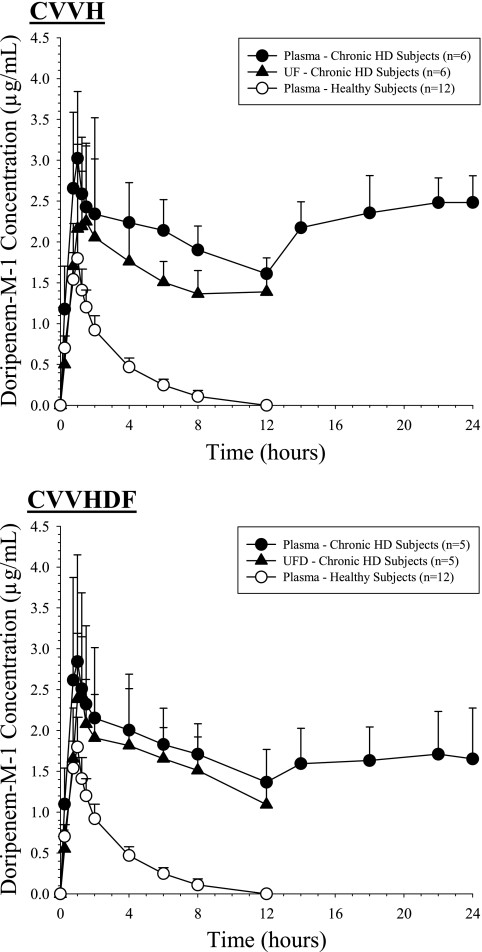
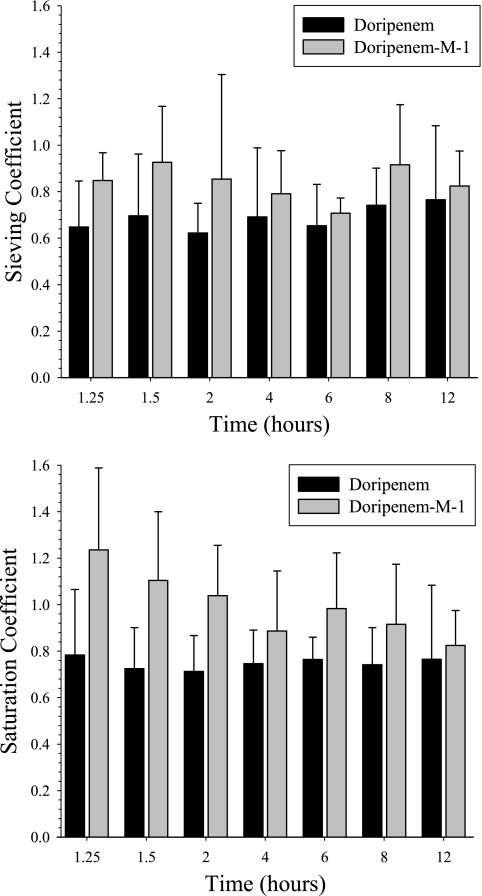
The pharmacokinetics, safety, and tolerability of a single 1-hour, 500-mg intravenous infusion of doripenem were assessed in dialysis-dependent subjects with stage 5 chronic kidney disease undergoing continuous renal replacement therapy (CRRT) via 12-hour continuous venovenous hemofiltration (CVVH) (n = 6) or continuous venovenous hemodiafiltration (CVVHDF) (n = 5). Healthy volunteers were also assessed (n = 12). Concentrations of doripenem and the primary metabolite doripenem-M-1 were measured in plasma and ultrafiltrate or ultrafiltrate/dialysate by a validated liquid chromatography-tandem mass spectrometry method. In dialysis-dependent subjects, levels of systemic exposure to doripenem and doripenem-M-1 were approximately 3- and 5-fold greater, respectively, than those in healthy subjects: for doripenem, 98 μg·h/ml for CVVH and 77 μg·h/ml for CVVHDF versus 32 μg·h/ml for healthy subjects, and for doripenem-M-1, 24 μg·h/ml for CVVH and 22 μg·h/ml for CVVHDF versus 4.7 μg·h/ml for healthy subjects. The mean sieving coefficients and saturation coefficients were >0.67 for both doripenem and doripenem-M-1. During CVVH and CVVHDF, respectively, the percentages of administered doripenem dose removed were 38% and 29%, and clearances of doripenem were 22 and 25 ml/min. Both CVVH and CVVHDF efficiently removed doripenem and doripenem-M-1. Despite significant removal of drug by CVVH and CVVHDF, a single 1-hour, 500-mg doripenem infusion produced significantly higher plasma concentrations of doripenem, higher systemic exposure (area under the plasma concentration-time curve from time zero to 12 h after the start of infusion [AUC(0-12)]), and longer half-life (t(1/2)) in subjects receiving CVVH or CVVHDF than in healthy volunteers. The recovery of drug in ultrafiltrate and ultrafiltrate/dialysate and the enhanced rate of reduction of plasma concentrations indicate that CVVH and CVVHDF significantly augmented residual total body clearance of doripenem in subjects receiving CRRT. Doripenem dosage regimens for patients receiving CRRT thus need to be adjusted.
Figures
References
-
- Aronoff, G. R., et al. 2007. Drug prescribing in renal failure: dosing guidelines for adults, 5th ed. American College of Physicians, Philadelphia, PA. - PubMed
-
- Bellomo, R., et al. 2009. Intensity of continuous renal-replacement therapy in critically ill patients. N. Engl. J. Med. 361:1627-1638. - PubMed
-
- Bugge, J. F. 2001. Pharmacokinetics and drug dosing adjustments during continuous venovenous hemofiltration or hemodiafiltration in critically ill patients. Acta Anaesthesiol. Scand. 45:929-934. - PubMed
-
- Burkhardt, O., et al. 2009. Pharmacokinetics of ertapenem in critically ill patients with acute renal failure undergoing extended daily dialysis. Nephrol. Dial. Transplant. 24:267-271. - PubMed
-
- Cerda, J., and C. Ronco. 2009. Modalities of continuous renal replacement therapy: technical and clinical considerations. Semin. Dial. 22:114-122. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
