

Development of lifetime comorbidity in the World Health Organization world mental health surveys
- PMID: 21199968
- PMCID: PMC3057480
- DOI: 10.1001/archgenpsychiatry.2010.180
Development of lifetime comorbidity in the World Health Organization world mental health surveys
Abstract
Context: Although numerous studies have examined the role of latent variables in the structure of comorbidity among mental disorders, none has examined their role in the development of comorbidity.
Objective: To study the role of latent variables in the development of comorbidity among 18 lifetime DSM-IV disorders in the World Health Organization World Mental Health Surveys.
Design: Nationally or regionally representative community surveys.
Setting: Fourteen countries.
Participants: A total of 21 229 survey respondents.
Main outcome measures: First onset of 18 lifetime DSM-IV anxiety, mood, behavior, and substance disorders assessed retrospectively in the World Health Organization Composite International Diagnostic Interview.
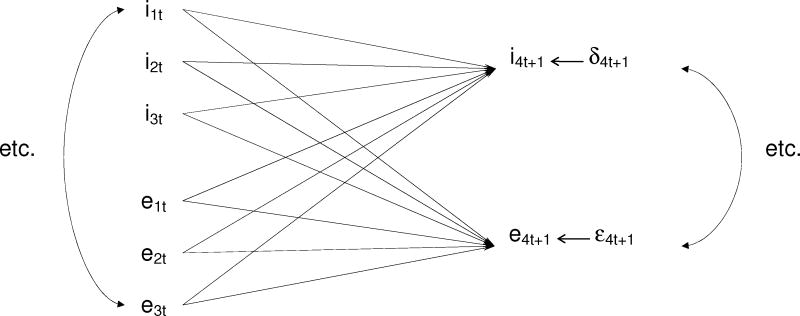
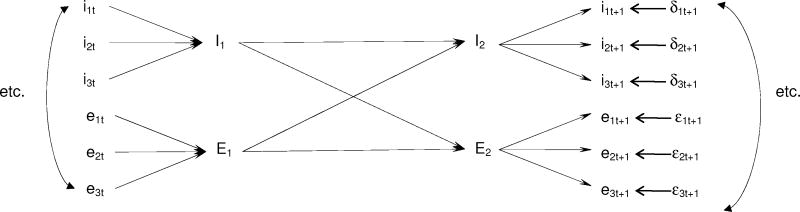
Results: Separate internalizing (anxiety and mood disorders) and externalizing (behavior and substance disorders) factors were found in exploratory factor analysis of lifetime disorders. Consistently significant positive time-lagged associations were found in survival analyses for virtually all temporally primary lifetime disorders predicting subsequent onset of other disorders. Within-domain (ie, internalizing or externalizing) associations were generally stronger than between-domain associations. Most time-lagged associations were explained by a model that assumed the existence of mediating latent internalizing and externalizing variables. Specific phobia and obsessive-compulsive disorder (internalizing) and hyperactivity and oppositional defiant disorders (externalizing) were the most important predictors. A small number of residual associations remained significant after controlling the latent variables.
Conclusions: The good fit of the latent variable model suggests that common causal pathways account for most of the comorbidity among the disorders considered herein. These common pathways should be the focus of future research on the development of comorbidity, although several important pairwise associations that cannot be accounted for by latent variables also exist that warrant further focused study.
Figures
Comment in
-
A dimensional-spectrum model of psychopathology: progress and opportunities.Arch Gen Psychiatry. 2011 Jan;68(1):10-1. doi: 10.1001/archgenpsychiatry.2010.188. Arch Gen Psychiatry. 2011. PMID: 21199961 No abstract available.
References
-
- Demyttenaere K, Bruffaerts R, Posada-Villa J, Gasquet I, Kovess V, Lepine JP, Angermeyer MC, Bernert S, de Girolamo G, Morosini P, Polidori G, Kikkawa T, Kawakami N, Ono Y, Takeshima T, Uda H, Karam EG, Fayyad JA, Karam AN, Mneimneh ZN, Medina-Mora ME, Borges G, Lara C, de Graaf R, Ormel J, Gureje O, Shen Y, Huang Y, Zhang M, Alonso J, Haro JM, Vilagut G, Bromet EJ, Gluzman S, Webb C, Kessler RC, Merikangas KR, Anthony JC, Von Korff MR, Wang PS, Brugha TS, Aguilar-Gaxiola S, Lee S, Heeringa S, Pennell BE, Zaslavsky AM, Ustun TB, Chatterji S. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization World Mental Health surveys. JAMA. 2004;291(21):2581–2590. - PubMed
-
- Krueger RF. The structure of common mental disorders. Arch Gen Psychiatry. 1999;56(10):921–926. - PubMed
-
- Cox BJ, Swinson RP. Instrument to assess depersonalization-derealization in panic disorder. Depress Anxiety. 2002;15(4):172–175. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 DA016558/DA/NIDA NIH HHS/United States
- U01-MH60220/MH/NIMH NIH HHS/United States
- R03 TW006481/TW/FIC NIH HHS/United States
- R01-MH069864/MH/NIMH NIH HHS/United States
- U01 MH060220/MH/NIMH NIH HHS/United States
- R13-MH066849/MH/NIMH NIH HHS/United States
- R01 MH070884/MH/NIMH NIH HHS/United States
- U13 MH066849/MH/NIMH NIH HHS/United States
- R13 MH066849/MH/NIMH NIH HHS/United States
- R01 MH069864/MH/NIMH NIH HHS/United States
- R01MH070884/MH/NIMH NIH HHS/United States
- K05 DA015799/DA/NIDA NIH HHS/United States
- R03-TW006481/TW/FIC NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
