

Comparison of a clinical prediction rule and a LAM antigen-detection assay for the rapid diagnosis of TBM in a high HIV prevalence setting
- PMID: 21203513
- PMCID: PMC3008727
- DOI: 10.1371/journal.pone.0015664
Comparison of a clinical prediction rule and a LAM antigen-detection assay for the rapid diagnosis of TBM in a high HIV prevalence setting
Abstract
Background/objective: The diagnosis of tuberculous meningitis (TBM) in resource poor TB endemic environments is challenging. The accuracy of current tools for the rapid diagnosis of TBM is suboptimal. We sought to develop a clinical-prediction rule for the diagnosis of TBM in a high HIV prevalence setting, and to compare performance outcomes to conventional diagnostic modalities and a novel lipoarabinomannan (LAM) antigen detection test (Clearview-TB®) using cerebrospinal fluid (CSF).
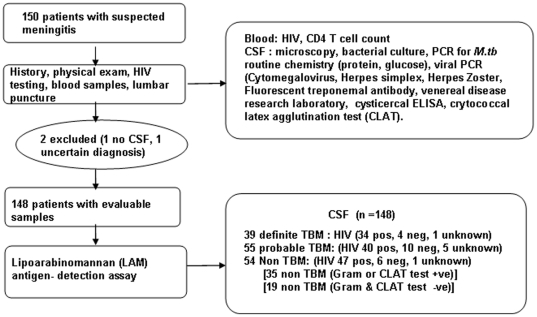
Methods: Patients with suspected TBM were classified as definite-TBM (CSF culture or PCR positive), probable-TBM and non-TBM.
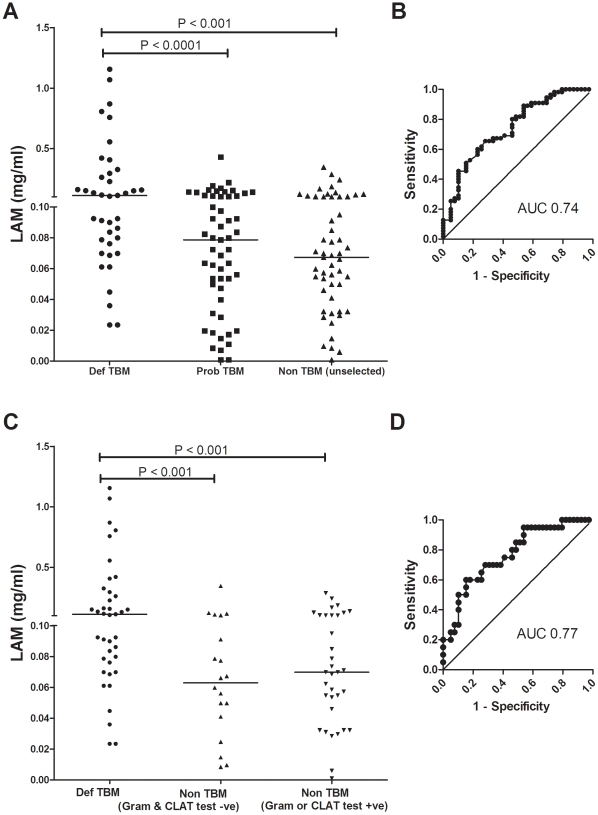
Results: Of the 150 patients, 84% were HIV-infected (median [IQR] CD4 count = 132 [54; 241] cells/µl). There were 39, 55 and 54 patients in the definite, probable and non-TBM groups, respectively. The LAM sensitivity and specificity (95%CI) was 31% (17;48) and 94% (85;99), respectively (cut-point ≥ 0.18). By contrast, smear-microscopy was 100% specific but detected none of the definite-TBM cases. LAM positivity was associated with HIV co-infection and low CD4 T cell count (CD4<200 vs. >200 cells/µl; p = 0.03). The sensitivity and specificity in those with a CD4<100 cells/µl was 50% (27;73) and 95% (74;99), respectively. A clinical-prediction rule ≥ 6 derived from multivariate analysis had a sensitivity and specificity (95%CI) of 47% (31;64) and 98% (90;100), respectively. When LAM was combined with the clinical-prediction-rule, the sensitivity increased significantly (p<0.001) to 63% (47;68) and specificity remained high at 93% (82;98).
Conclusions: Despite its modest sensitivity the LAM ELISA is an accurate rapid rule-in test for TBM that has incremental value over smear-microscopy. The rule-in value of LAM can be further increased by combination with a clinical-prediction rule, thus enhancing the rapid diagnosis of TBM in HIV-infected persons with advanced immunosuppression.
Conflict of interest statement
Figures
References
-
- World Health Organisation. Global tuberculosis control: Surveillance, planning, financing. Available . 2008. http://www.who.int/tb/publications/global_report/2008/en/index.html.
-
- Centers for Disease Control. Atlanta, GA: Centers for Disease Control and Prevention; 2005. Extrapulmonary tuberculosis cases and percentages by site of disease: reporting areas. Available: www.cdc.gov/tb/surv/surv2005/PDF/table27.pdf.
-
- Braunwald E, Fauchi AS, Kasper DL, Hauser SL, Longo DL, et al. Harrisons's Principles of Internal Medicine 15th Edition: McGraw-Hill p1028. 2001
-
- Ozbay B, Uzun K. Extrapulmonary tuberculosis in high prevalence of tuberculosis and low prevalence of HIV. Clin Chest Med. 2002;23:351–354. - PubMed
-
- Phypers M, Harris T, Power C. CNS tuberculosis: a longitudinal analysis of epidemiological and clinical features. Int J Tuberc Lung Dis. 2006;10:99–103. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
