

Isolated cerebellar mucormycosis, slowly progressive over 1 year in an immunocompetent patient
- PMID: 21206542
- PMCID: PMC3011109
- DOI: 10.4103/2152-7806.73800
Isolated cerebellar mucormycosis, slowly progressive over 1 year in an immunocompetent patient
Abstract
Background: Mucormycosis is a rare, aggressive fungal disease with high mortality, typically presenting as rhinosinusitis in immunocompromised patients.
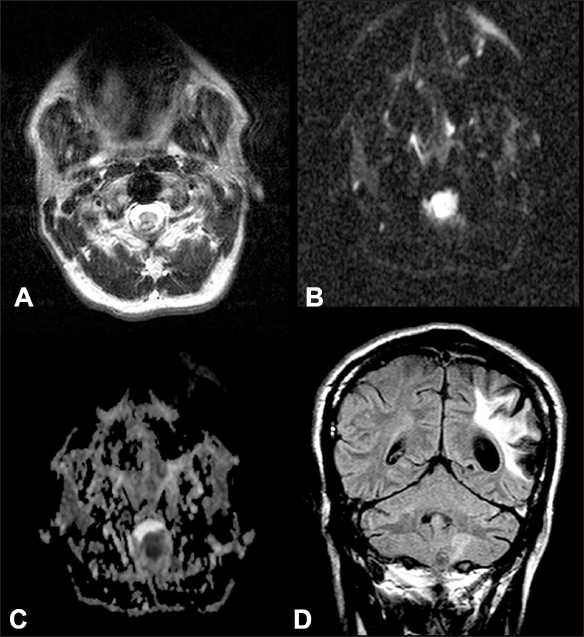
Case description: A 43-year-old man with a history of intravenous drug use, Hepatitis C, and no evidence of immunocompromise presented with worsening balance problems. He had received intravenous antibiotics 2.5 years earlier for local infection after injecting heroin into a neck vein. Imaging studies revealed a lesion, likely of neoplastic origin. At resection, purulent fluid sampled by neuropathology revealed right-angled, branching hyphae, suggesting mucormycosis. No further resection was performed, no other disease sites were found, and HIV findings were negative. Two weeks postoperatively, he developed renal failure; intravenous antifungal treatment and hemodialysis were discontinued. When kidney function recovered 2 weeks later, he declined additional treatment.
Conclusion: In our immunocompetent patient, both the location of the infection in the posterior fossa and its slowly progressive characteristic were unique variations of this typically aggressive disease.
Keywords: Fungal; immunocompetent; infection; intravenous drug abuse; mucormycosis; rhinocerebral.
Figures


References
-
- Abbas Z, Jafri W, Rasool S, Abid S, Hameed I. Mucormycosis in patients with complicated cirrhosis. Singapore Med J. 2007;48:69–73. - PubMed
-
- Adler CH, Stern MB, Brooks ML. Parkinsonism secondary to bilateral striatal fungal abscesses. Mov Disord. 1989;4:333–7. - PubMed
-
- Agarwal R, Kumar V, Gupta D. Pulmonary mucormycosis: Two of a kind. Eur J Intern Med. 2006;17:63–5. - PubMed
-
- Ameen M, Arenas R, Martinez-Luna E, Reyes M, Zacarias R. The emergence of mucormycosis as an important opportunistic fungal infection: Five cases presenting to a tertiary referral center for mycology. Int J Dermatol. 2007;46:380–4. - PubMed
-
- Blazquez R, Pinedo A, Cosín J, Miralles P, Lacruz C, Bouza E. Nonsurgical cure of isolated cerebral mucormycosis in an intravenous drug user. Eur J Clin Microbiol Infect Dis. 1996;15:598–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
