

Long delays and missed opportunities in diagnosing smear-positive pulmonary tuberculosis in Kampala, Uganda: a cross-sectional study
- PMID: 21206746
- PMCID: PMC3012078
- DOI: 10.1371/journal.pone.0014459
Long delays and missed opportunities in diagnosing smear-positive pulmonary tuberculosis in Kampala, Uganda: a cross-sectional study
Abstract
Background: Early detection and treatment of tuberculosis cases are the hallmark of successful tuberculosis control. We conducted a cross-sectional study at public primary health facilities in Kampala city, Uganda to quantify diagnostic delay among pulmonary tuberculosis (PTB) patients, assess associated factors, and describe trajectories of patients' health care seeking.
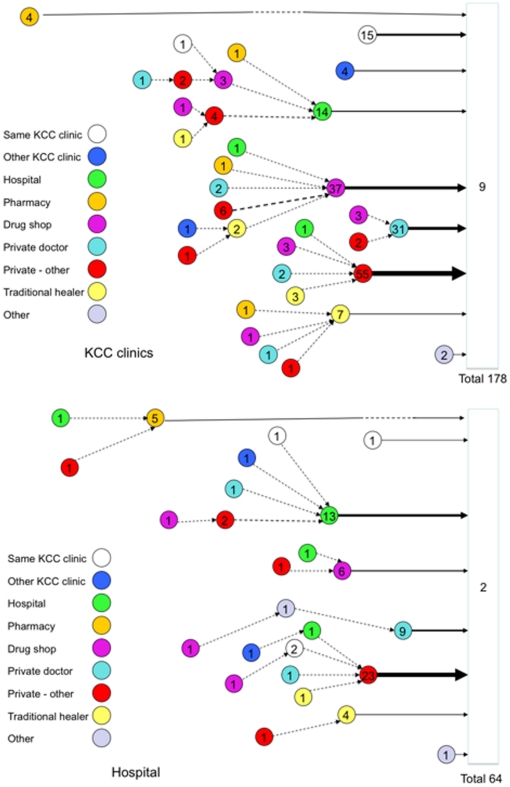
Methodology/principal findings: Semi-structured interviews with new smear-positive PTB patients (≥ 15 years) registered for treatment. Between April 2007 and April 2008, 253 patients were studied. The median total delay was 8 weeks (IQR 4-12), median patient delay was 4 weeks (inter-quartile range [IQR] 1-8) and median health service delay was 4 weeks (IQR 2-8). Long total delay (>14 weeks) was observed for 61/253 (24.1%) of patients, long health service delay (>6 weeks) for 71/242 (29.3%) and long patient delay (>8 weeks) for 47/242 (19.4%). Patients who knew that TB was curable were less likely to have long total delay (adjusted Odds Ratio [aOR] 0.28; 95%CI 0.11-0.73) and long patient delay (aOR 0.36; 95%CI 0.13-0.97). Being female (aOR 1.98; 95%CI 1.06-3.71), staying for more than 5 years at current residence (aOR 2.24 95%CI 1.18-4.27) and having been tested for HIV before (aOR 3.72; 95%CI 1.42-9.75) was associated with long health service delay. Health service delay contributed 50% of the total delay. Ninety-one percent (231) of patients had visited one or more health care providers before they were diagnosed, for an average (median) of 4 visits (range 1-30). All but four patients had systemic symptoms by the time the diagnosis of TB was made.
Conclusions/significance: Diagnostic delay among tuberculosis patients in Kampala is common and long. This reflects patients waiting too long before seeking care and health services waiting until systemic symptoms are present before examining sputum smears; this results in missed opportunities for diagnosis.
Conflict of interest statement
Figures

References
-
- World Health Organization. Global Tuberculosis Control: Epidemiology, Strategy, Financing. 2009. Geneva.
-
- World Health Organization. Treatment of tuberculosis: Guidelines for National Programmes. 2003. Geneva.
-
- Ward HA, Marciniuk DD, Pahwa P, Hoeppnner VH. Extent of pulmonary tuberculosis in patients diagnosed by active compared to passive case finding. Int J Tuberc Lung Dis. 2004;8:593–597. - PubMed
-
- Bustamante-Montes LP, Escobar-Mesa A, Borja-Aburto VH, Gomez-Munoz A, Becerra-Posad F. Predictors of death from pulmonary tuberculosis: the case of Veracruz, Mexico. Int. J Tuberc Lung Dis. 2000;4:208–215. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
