

A porcine model of acute, haematogenous, localized osteomyelitis due to Staphylococcus aureus: a pathomorphological study
- PMID: 21208278
- PMCID: PMC3040840
- DOI: 10.1111/j.1600-0463.2010.02700.x
A porcine model of acute, haematogenous, localized osteomyelitis due to Staphylococcus aureus: a pathomorphological study
Abstract
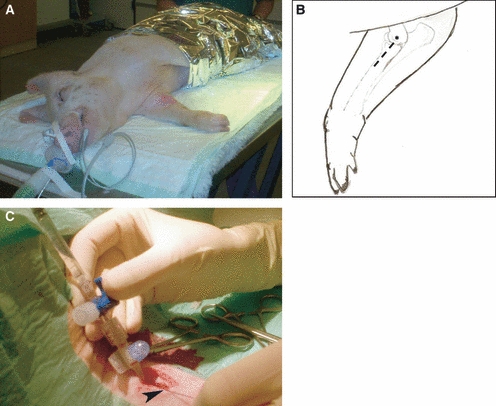
A porcine model of acute, haematogenous, localized osteomyelitis was established. Serial dilutions of Staphylococcus aureus [5-50-500-5000-50 000 CFU/kg body weight (BW) suspended in saline or saline alone] were inoculated into the right brachial artery of pigs (BW 15 kg) separated into six groups of two animals. During the infection, blood was collected for cultivation, and after the animals were killed from day 5 to 15, they were necropsied and tissues were sampled for histopathology. Animals receiving ≤500 CFU/kg BW were free of lesions. Pigs inoculated with 5000 and 50 000 CFU/kg BW only developed microabscesses in bones of the infected legs. In the centre of microabscesses, S. aureus was regularly demonstrated together with necrotic neutrophils. Often, bone lesions resulted in trabecular osteonecrosis. The present localized model of acute haematogenous osteomyelitis revealed a pattern of development and presence of lesions similar to the situation in children. Therefore, this model should be reliably applied in studies of this disease with respect to e.g. pathophysiology and pathomorphology. Moreover, because of the regional containment of the infection to a defined number of bones, the model should be applicable also for screening of new therapy strategies.
© 2010 The Authors. APMIS © 2010 APMIS.
Figures
 ).
).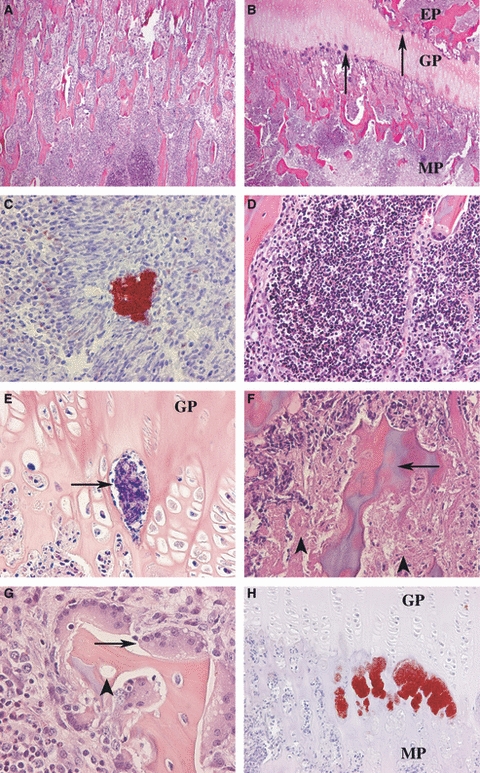
 ), H&E. (G) Trabeculae with empty lacunae (
), H&E. (G) Trabeculae with empty lacunae ( ) were typically surrounded by bone resorbing osteoclasts (→), H&E. (H) Multiple S. aureus bacteria were often identified in connection with the capillary loops at the junction between the growth plate (GP) and the metaphysis (MP). Immunostaining for S. aureus.
) were typically surrounded by bone resorbing osteoclasts (→), H&E. (H) Multiple S. aureus bacteria were often identified in connection with the capillary loops at the junction between the growth plate (GP) and the metaphysis (MP). Immunostaining for S. aureus.References
-
- Goergens ED, McEvoy A, Watson M, Barrett IR. Acute osteomyelitis and septic arthritis in children. J Paediatr Child Health. 2005;41:59–62. - PubMed
-
- Lazzarini L, Mader JT, Calhoun JH. Osteomyelitis in long bones. J Bone Joint Surg Am. 2004;86-A:2305–18. - PubMed
-
- Gelfand MS, Cleveland KO, Heck RK, Goswami R. Pathological fracture in acute osteomyelitis of long bones secondary to community-acquired methicillin-resistant Staphylococcus aureus: two cases and review of the literature. Am J Med Sci. 2006;332:357–60. - PubMed
-
- Perlman MH, Patzakis MJ, Kumar PJ, Holtom P. The incidence of joint involvement with adjacent osteomyelitis in pediatric patients. J Pediatr Orthop. 2000;20:40–3. - PubMed
-
- Kao HC, Huang YC, Chiu CH, Chang LY, Lee ZL, Chung PW, et al. Acute hematogenous osteomyelitis and septic arthritis in children. J Microbiol Immunol Infect. 2003;36:260–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
