

Long-term outcome of adolescent depression initially resistant to selective serotonin reuptake inhibitor treatment: a follow-up study of the TORDIA sample
- PMID: 21208583
- PMCID: PMC3070064
- DOI: 10.4088/JCP.09m05885blu
Long-term outcome of adolescent depression initially resistant to selective serotonin reuptake inhibitor treatment: a follow-up study of the TORDIA sample
Erratum in
-
Correction.J Clin Psychiatry. 2019 Oct 23;80(5):19lcx13039. doi: 10.4088/JCP.19lcx13039. J Clin Psychiatry. 2019. PMID: 31556973
Abstract
Background: We examined the long-term outcome of participants in the Treatment of SSRI-Resistant Depression in Adolescents (TORDIA) study, a randomized trial of 334 adolescents (aged 12-18 years) with DSM-IV-defined major depressive disorder initially resistant to selective serotonin reuptake inhibitor (SSRI) treatment who were subsequently treated for 12 weeks with another SSRI, venlafaxine, another SSRI + cognitive-behavioral therapy (CBT), or venlafaxine + CBT. Responders then continued with the same treatment through week 24, while nonresponders were given open treatment.
Method: For the current study, patients were reassessed 48 (n = 116) and 72 (n = 130) weeks from intake. Data were gathered from February 2001 to February 2007. Standardized diagnostic interviews and measures of depression, suicidal ideation, related psychopathology, and level of functioning were periodically administered. Remission was defined as ≥ 3 weeks with ≤ 1 clinically significant symptom and no associated functional impairment (score of 1 on the adolescent version of the Longitudinal Interval Follow-Up Evaluation [A-LIFE]), and relapse, as ≥ 2 weeks with probable or definite depressive disorder (score of 3 or 4 on the A-LIFE). Mixed-effects regression models were applied to estimate remission, relapse, and functional recovery.
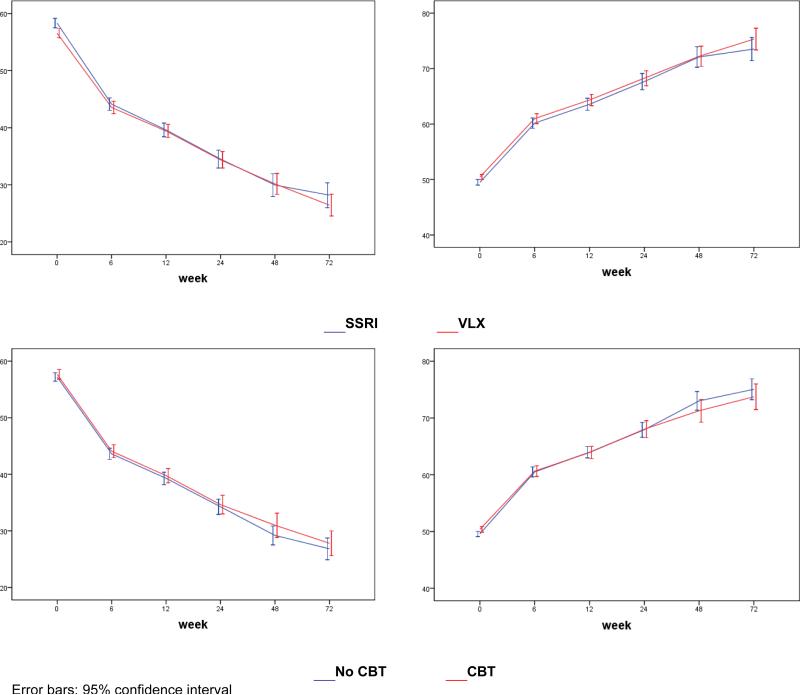
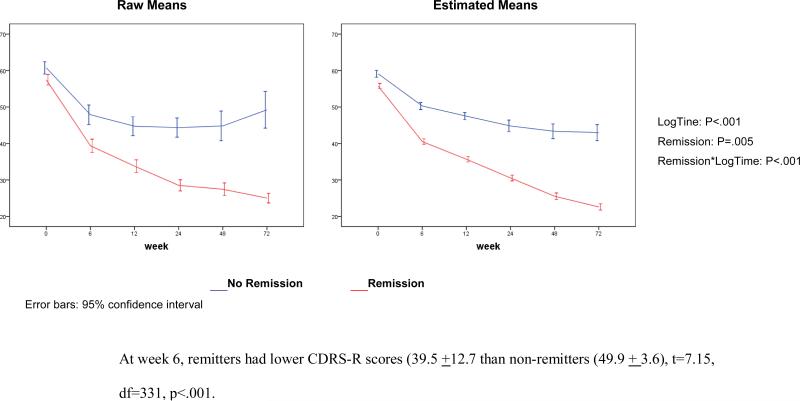
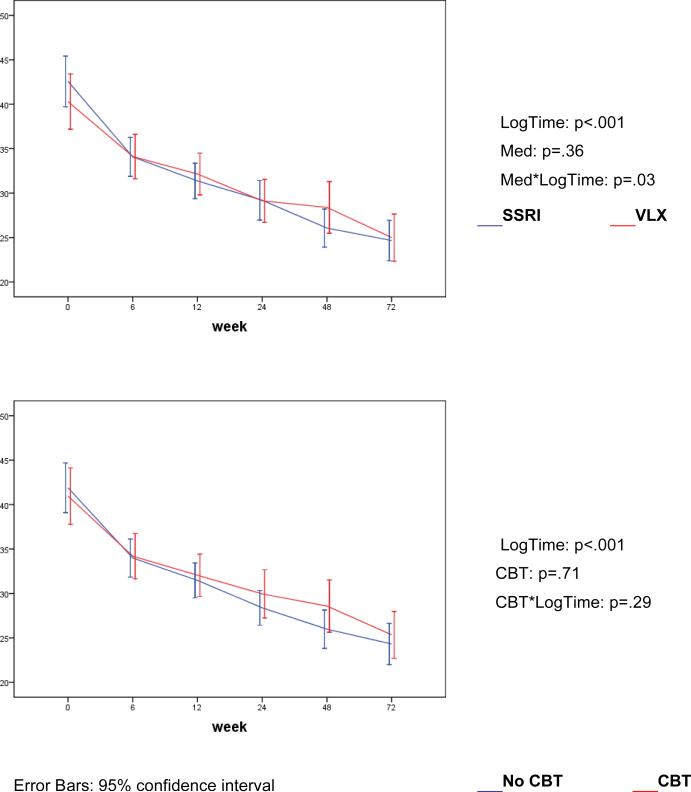
Results: By 72 weeks, an estimated 61.1% of the randomized youths had reached remission. Randomly assigned treatment (first 12 weeks) did not influence remission rate or time to remission, but the group assigned to SSRIs had a more rapid decline in self-reported depressive symptoms and suicidal ideation than those assigned to venlafaxine (P < .03). Participants with more severe depression, greater dysfunction, and alcohol or drug use at baseline were less likely to remit. The depressive symptom trajectory of the remitters diverged from that of nonremitters by the first 6 weeks of treatment (P < .001). Of the 130 participants in remission at week 24, 25.4% relapsed in the subsequent year.
Conclusions: While most adolescents achieved remission, more than one-third did not, and one-fourth of remitted patients experienced a relapse. More effective interventions are needed for patients who do not show robust improvement early in treatment.
Trial registration: clinicaltrials.gov Identifier: NCT00018902.
© Copyright 2011 Physicians Postgraduate Press, Inc.
Figures
Comment in
-
Impact of mood disorders.J Clin Psychiatry. 2011 Mar;72(3):376-7. doi: 10.4088/JCP.11f06857. J Clin Psychiatry. 2011. PMID: 21450155 No abstract available.
-
Most adolescents achieve longer term remission from major depressive disorder regardless of type of short-term second-line treatment.Evid Based Ment Health. 2011 Aug;14(3):85. doi: 10.1136/ebmh.14.3.85. Evid Based Ment Health. 2011. PMID: 21764884 No abstract available.
References
-
- Kennard B, Silva SG, Tonev S, Rohde P, Hughes JL, Vitiello B, Kratochvil CJ, Curry JF, Emslie GJ, Reinecke M, March J. Remission and recovery in the Treatment for Adolescents with Depression Study (TADS): acute and long-term outcomes. J Am Acad Child Adolesc Psychiatry. 2009;48:186–195. - PMC - PubMed
-
- TADS Team The Treatment for Adolescents With Depression Study (TADS): outcomes over 1 year of naturalistic follow-up. Am J Psychiatry. 2009;166:1141–1149. - PubMed
-
- Brent D, Emslie G, Clarke G, Wagner K, Asarnow J, Keller M, Vitiello B, Ritz L, Satish Iyengar S, Abebe K, Birmaher B, Ryan N, Kennard B, Hughes C, DeBar L, McCracken J, Strober M, Suddath R, Spirito A, Leonard H, Porta G, Onorato M, Zelazny J. The Treatment of Adolescents with SSRI-Resistant Depression (TORDIA). A comparison of switch to venlafaxine or to another SSRI, with or without additional cognitive behavioral therapy. JAMA. 2008;299:901–13. - PMC - PubMed
-
- Asarnow JR, Emslie G, Clarke G, Wagner KD, Spirito A, Vitiello B, Iyengar S, Shamseddeen W, Ritz L, Birmaher B, Ryan N, Kennard B, Mayes T, Debar L, McCracken J, Strober M, Suddath R, Leonard H, Porta G, Keller M, Brent D. Treatment of Selective Serotonin Reuptake Inhibitor-Resistant-Depression in Adolescents: predictors and moderators of Treatment Response. J Am Acad Child Adolesc Psychiatry. 2009;48:330–339. - PMC - PubMed
-
- Brent DA, Emslie GJ, Clarke GN, Asarnow J, Spirito A, Ritz L, Vitiello B, Iyengar S, Birmaher B, Ryan ND, Zelazny J, Onorato M, Kennard B, Mayes TL, Debar LL, McCracken JT, Strober M, Suddath R, Leonard H, Porta G, Keller MB. Predictors of spontaneous and systematically assessed suicidal adverse events in the Treatment of SSRI-Resistant Depression in Adolescents (TORDIA) study. Am J Psychiatry. 2009;166:418–426. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
