

Clinical outcome of HIV-infected patients with discordant virological and immunological response to antiretroviral therapy
- PMID: 21208929
- PMCID: PMC3130441
- DOI: 10.1093/jinfdis/jiq055
Clinical outcome of HIV-infected patients with discordant virological and immunological response to antiretroviral therapy
Abstract
Background: A subgroup of human immunodeficiency virus type 1 (HIV-1)-infected patients with severe immunodeficiency show persistently low CD4+ cell counts despite sustained viral suppression. It is unclear whether this immuno-virological discordance translates into an increased risk for clinical events.
Methods: Data analysis from a large multicenter cohort incorporating 14,433 HIV-1-infected patients in Germany. Treatment-naive patients beginning antiretroviral therapy (ART) with CD4+ cell counts <200 cells/μL who achieved complete and sustained viral suppression <50 copies/mL (n = 1318) were stratified according to the duration of immuno-virological discordance (failure to achieve a CD4+ cell count ≥200 cells/μL). Groups were compared by descriptive and Poisson statistics. The time-varying discordance status was analyzed in a multivariable Cox model.
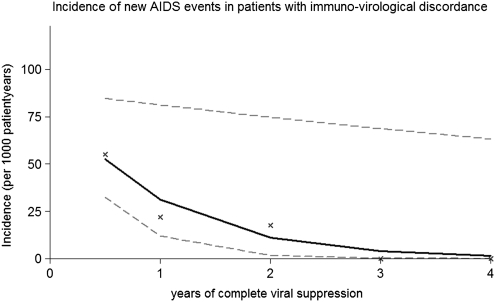
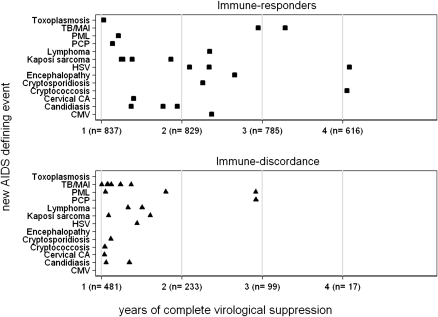
Results: During a total of 5038 person years of follow-up, 42 new AIDS events occurred. The incidence rate of new AIDS events was highest in the initial 6 months of complete viral suppression (immuno-virological discordance group, 55.06; 95% confidence interval [CI], 30.82-90.82; and immune responder group, 24.54; 95% CI, 10.59-48.35) and decreased significantly by 65% per year in patients with immuno-virological discordance (incidence risk ratio, 0.35; 95% CI, 0.14-0.92; P = .03). Immuno-virological discordance and prior AIDS diagnosis were independently associated with new AIDS events (hazard ratio, 3.10; 95% CI, 1.09-8.82; P = .03).
Conclusion: Compared with immune responders, patients with immuno-virological discordance seem to remain at increased risk for AIDS. Absolute risk is greatly reduced after the first 6 months of complete viral suppression.
Figures
References
-
- Mocroft A, Vella S, Benfield TL, et al. Changing patterns of mortality across Europe in patients infected with HIV-1. EuroSIDA Study Group. Lancet. 1998;352:1725–30. - PubMed
-
- Palella FJ, Jr., Delaney KM, Moorman AC, et al. Declining morbidity mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–60. - PubMed
-
- Mellors JW, Munoz A, Giorgi JV, et al. Plasma viral load CD4+ lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med. 1997;126:946–54. - PubMed
-
- Hughes MD, Daniels MJ, Fischl MA, Kim S, Schooley RT. CD4+ cell count as a surrogate endpoint in HIV clinical trials: a meta-analysis of studies of the AIDS Clinical Trials Group. AIDS. 1998;12:1823–32. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
