

Randomized phase II trial of sulindac, atorvastatin, and prebiotic dietary fiber for colorectal cancer chemoprevention
- PMID: 21209397
- PMCID: PMC3046804
- DOI: 10.1158/1940-6207.CAPR-10-0215
Randomized phase II trial of sulindac, atorvastatin, and prebiotic dietary fiber for colorectal cancer chemoprevention
Abstract
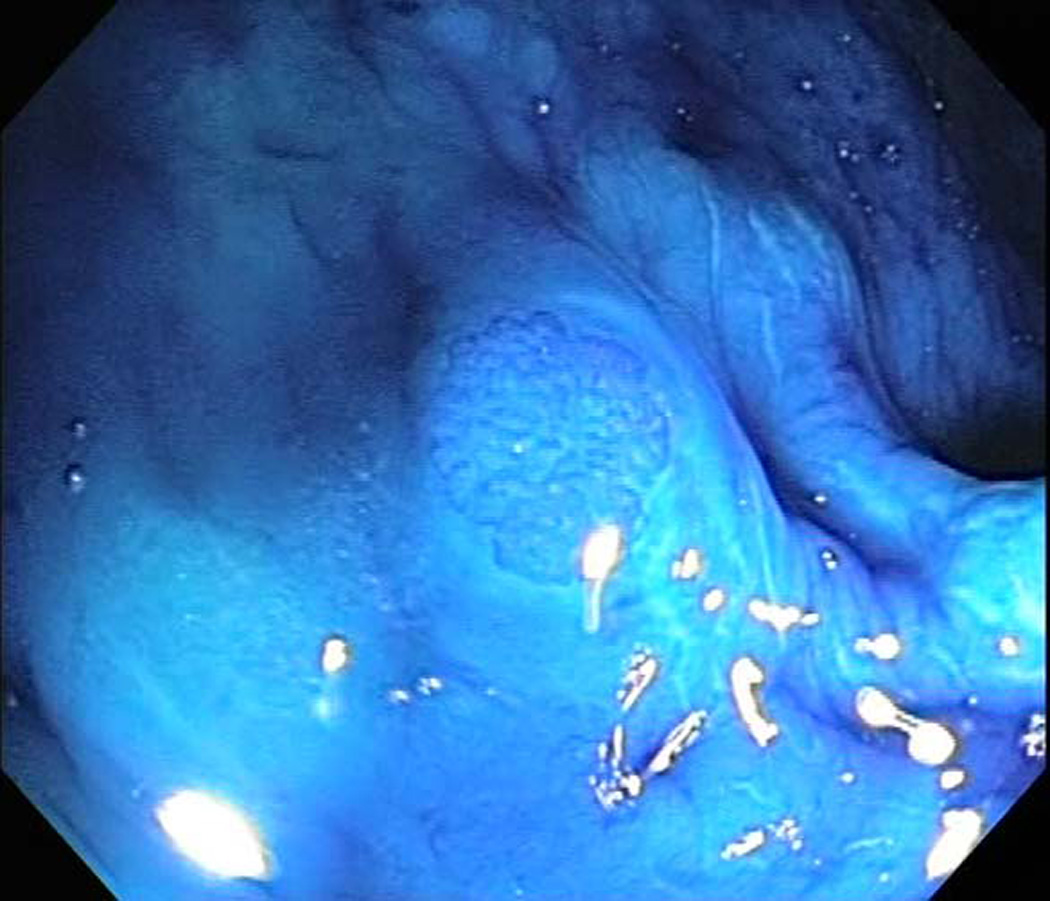
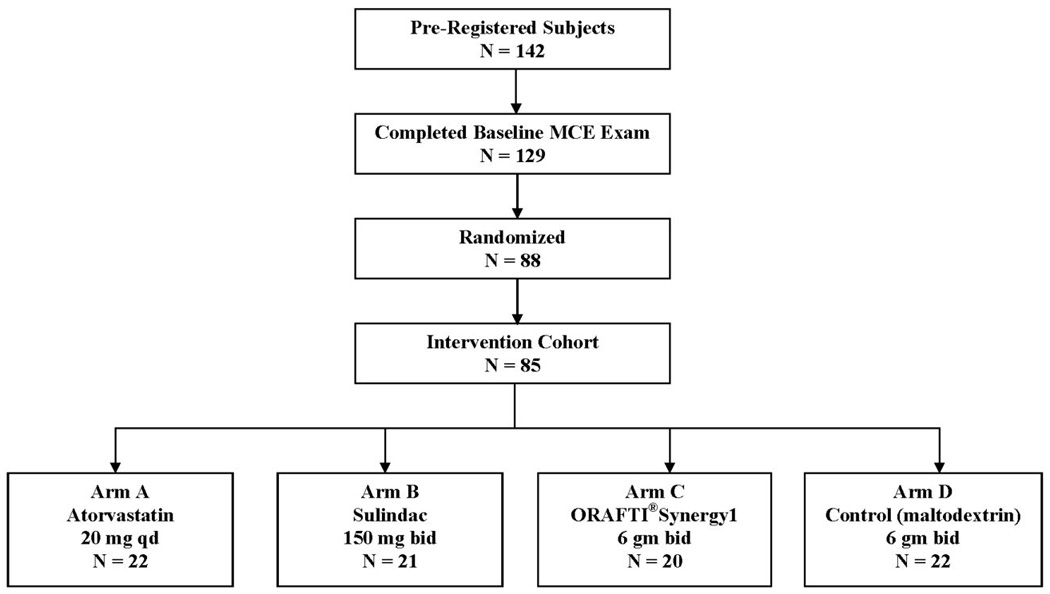
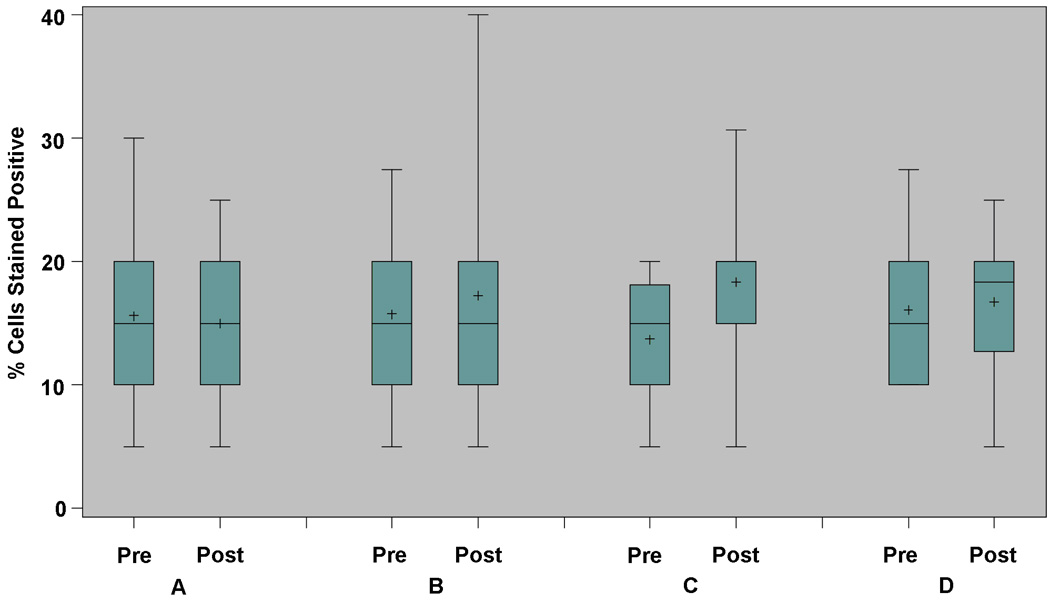
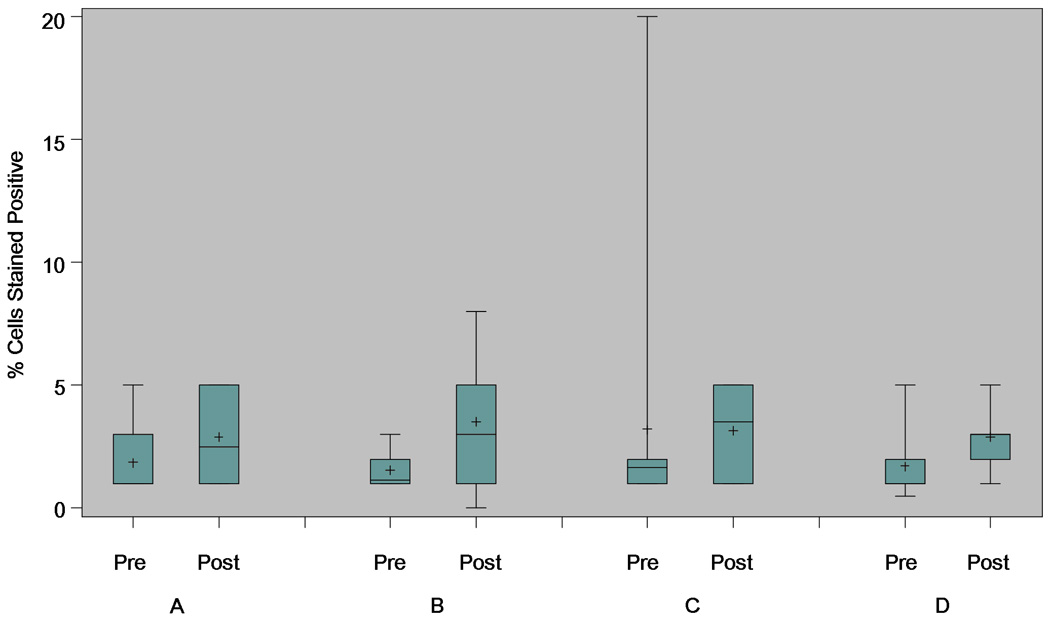
Sulindac, atorvastatin, or prebiotic dietary fiber may reduce colorectal cancer (CRC) risk. However, clinical trial data are currently limited. We conducted a randomized, phase II chemoprevention trial involving subjects 40 years or older, with previously resected colon cancer or multiple/advanced colorectal adenomas. Magnification chromoendoscopy (MCE) was performed to identify and characterize rectal aberrant crypt foci (ACF); eligibility criteria required five or more rectal ACFs at baseline. Intervention assignments were as follows: (a) atorvastatin 20 mg qd; (b) sulindac 150 mg bid; (c) oligofructose-enriched inulin (as ORAFTI®Synergy1) 6 gm bid; or (d) control (maltodextrin) 6 gm bid, for 6 months. Percent change in rectal ACF number (%ΔACF) within arm was the primary endpoint. Secondary endpoints included changes in proliferation (Ki67) and apoptosis (caspase-3), as measured from normal mucosa biopsy samples. Among 85 eligible randomized subjects, 76 (86%) completed the trial per protocol. The median (range) of rectal ACF was 9 (5-34) and 8 (0-37) at baseline and postintervention, respectively. The median (SD) for %ΔACF was 5.6 (-69% to 143%), -18.6 (-83% to 160%), -3.6 (-88% to 83%), and -10.0 (-100% to 117%) in the atorvastatin, sulindac, ORAFTI®Synergy1 and control arms, respectively. Neither within-arm (P = 0.12-0.59) nor between-arm (P = 0.30-0.92) comparisons of %ΔACF were statistically significant. The active and control interventions also seemed to have similar effects on mucosal proliferation and apoptosis (P > 0.05 for each comparison). Data from this multicenter, phase II trial do not provide convincing evidence of CRC risk reduction from 6-month interventions with atorvastatin, sulindac, or ORAFTI®Synergy1, although statistical power was limited by the relatively small sample size.
©2011 AACR.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- Herszenyi L, Farinati F, Miheller P, et al. Chemoprevention of colorectal cancer: feasibility in everyday practice? Eur J Cancer Prev. 2008;17:502–514. - PubMed
-
- Das D, Arber N, Jankowski JA. Chemoprevention of colorectal cancer. Digestion. 2007;76:51–67. - PubMed
-
- Hawk ET, Umar A, Viner JL. Colorectal cancer chemoprevention--an overview of the science. Gastroenterology. 2004;126:1423–1447. - PubMed
-
- Giardiello FM, Hamilton SR, Krush AJ, et al. Treatment of colonic and rectal adenomas with sulindac in familial adenomatous polyposis. N Engl J Med. 1993;328:1313–1316. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
