

A large web-based observer reliability study of early ischaemic signs on computed tomography. The Acute Cerebral CT Evaluation of Stroke Study (ACCESS)
- PMID: 21209901
- PMCID: PMC3012713
- DOI: 10.1371/journal.pone.0015757
A large web-based observer reliability study of early ischaemic signs on computed tomography. The Acute Cerebral CT Evaluation of Stroke Study (ACCESS)
Abstract
Background: Early signs of ischaemic stroke on computerised tomography (CT) scanning are subtle but CT is the most widely available diagnostic test for stroke. Scoring methods that code for the extent of brain ischaemia may improve stroke diagnosis and quantification of the impact of ischaemia.
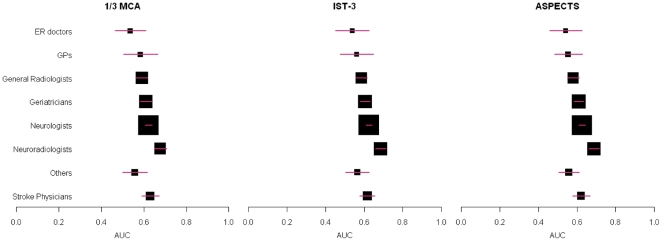
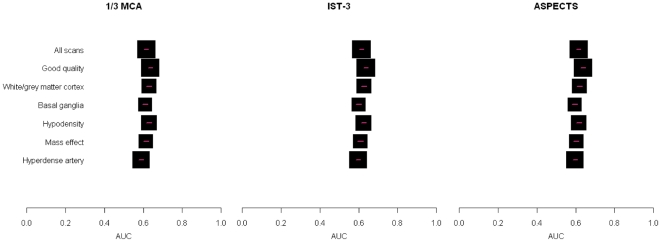
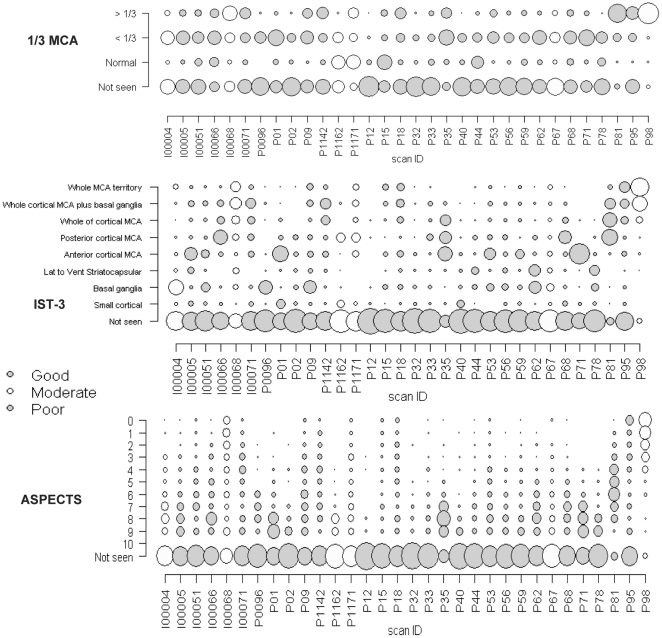
Methodology and principal findings: We showed CT scans from patients with acute ischaemic stroke (n = 32, with different patient characteristics and ischaemia signs) to doctors in stroke-related specialties world-wide over the web. CT scans were shown twice, randomly and blindly. Observers entered their scan readings, including early ischaemic signs by three scoring methods, into the web database. We compared observers' scorings to a reference standard neuroradiologist using area under receiver operator characteristic curve (AUC) analysis, Cronbach's alpha and logistic regression to determine the effect of scales, patient, scan and observer variables on detection of early ischaemic changes. Amongst 258 readers representing 33 nationalities and six specialties, the AUCs comparing readers with the reference standard detection of ischaemic signs were similar for all scales and both occasions. Being a neuroradiologist, slower scan reading, more pronounced ischaemic signs and later time to CT all improved detection of early ischaemic signs and agreement on the rating scales. Scan quality, stroke severity and number of years of training did not affect agreement.
Conclusions: Large-scale observer reliability studies are possible using web-based tools and inform routine practice. Slower scan reading and use of CT infarct rating scales improve detection of acute ischaemic signs and should be encouraged to improve stroke diagnosis.
Conflict of interest statement
Figures
References
-
- Kane I, Whiteley WN, Sandercock PA, Wardlaw JM. Availability of CT and MR for assessing patients with acute stroke. Cerebrovasc Dis. 2008;25:375–377. - PubMed
-
- Leys D, Ringelstein EB, Kaste M, Hacke W. Facilities available in European hospitals treating stroke patients. Stroke. 2007;38:2985–2991. - PubMed
-
- Hossmann KA, Schuier FJ. Experimental brain infarcts in cats. I. Pathophysiological observations. Stroke. 1980;11:583–592. - PubMed
-
- Dzialowski I, Klotz E, Goericke S, Doerfler A, Forsting M, et al. Ischemic brain tissue water content: CT monitoring during middle cerebral artery occlusion and reperfusion in rats. Radiology. 2007;243:720–726. - PubMed
