

The effect of tuberculosis on mortality in HIV positive people: a meta-analysis
- PMID: 21209936
- PMCID: PMC3012688
- DOI: 10.1371/journal.pone.0015241
The effect of tuberculosis on mortality in HIV positive people: a meta-analysis
Abstract
Background: Tuberculosis is a leading cause of death in people living with HIV (PLWH). We conducted a meta analysis to assess the effect of tuberculosis on mortality in people living with HIV.
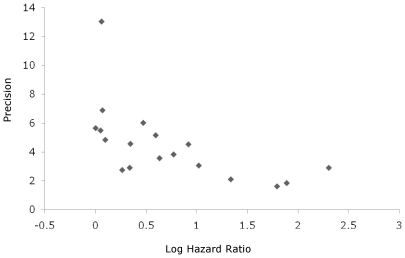
Methods: Meta-analysis of cohort studies assessing the effect of tuberculosis on mortality in PLWH. To identify eligible studies we systematically searched electronic databases (until December 2008), performed manual searches of citations from relevant articles, and reviewed conference proceedings. Multivariate hazard ratios (HR) of mortality in PLWH with and without tuberculosis, estimated in individual cohort studies, were pooled using random effect weighting according to "Der Simonian Laird method" if the p-value of the heterogeneity test was <0.05.
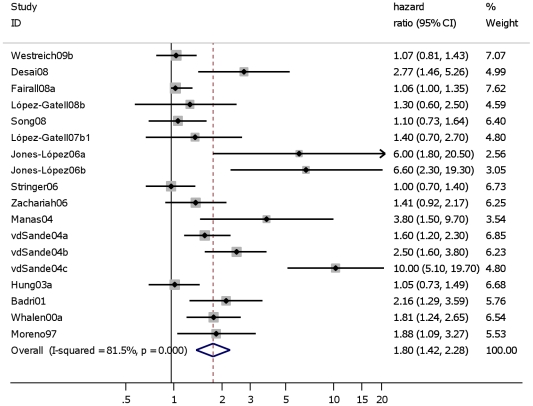
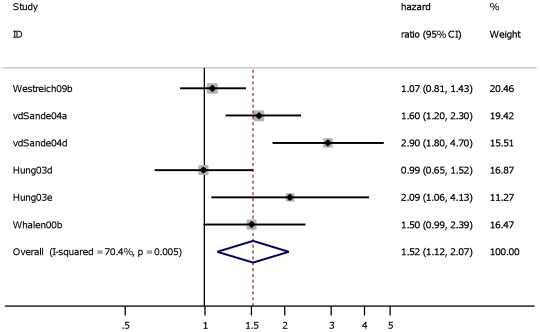
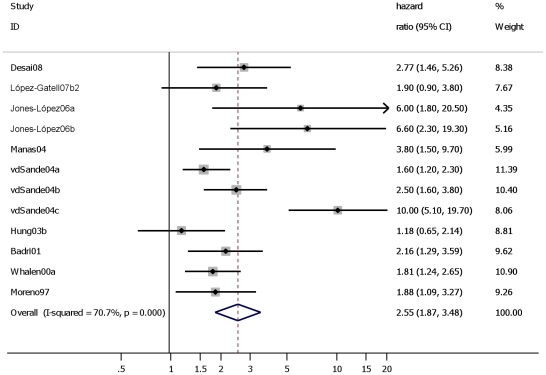
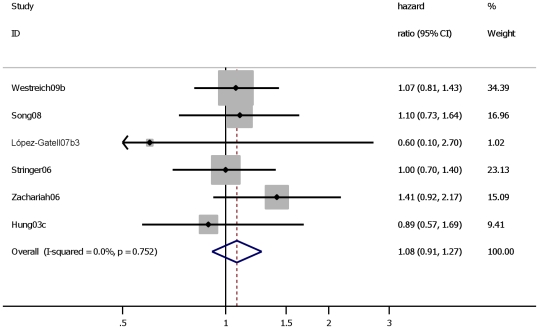
Results: Fifteen cohort studies were systematically retrieved. Pooled overall analysis of these 15 studies estimating the effect of tuberculosis on mortality in PLWH showed a Hazard Ratio (HR) of 1.8 (95% confidence interval (CI): 1.4-2.3). Subanalysis of 8 studies in which the cohort was not exposed to highly active antiretroviral therapy (HAART) showed an HR of 2.6 (95% CI: 1.8-3.6). Subanalysis of 6 studies showed that tuberculosis did not show an effect on mortality in PLWH exposed to HAART: HR 1.1 (95% CI: 0.9-1.3).
Conclusion: These results provide an indication of the magnitude of benefit to an individual that could have been expected if tuberculosis had been prevented. It emphasizes the need for additional studies assessing the effect of preventing tuberculosis or early diagnosis and treatment of tuberculosis in PLWH on reducing mortality. Furthermore, the results of the subgroup analyses in cohorts largely exposed to HAART provide additional support to WHO's revised guidelines, which include promoting the initiation of HAART for PLWH co-infected with tuberculosis. The causal effect of tuberculosis on mortality in PLWH exposed to HAART needs to be further evaluated once the results of more cohort studies become available.
Conflict of interest statement
Figures

References
-
- World Health Organization. Geneva; 2009. Global Tuberculosis Control: a short update to the 2009 report.
-
- Munsiff SS, Alpert PL, Gourevitch MN, Chang CJ, Klein RS. A prospective study of tuberculosis and HIV disease progression. J Acquir Immune Defic Syndr Hum Retrovirol. 1998;19:361–6. - PubMed
-
- Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med. 2003;163:1009–21. - PubMed
-
- Mendelson M. Diagnosing tuberculosis in HIV-infected patients: challenges and future prospects. Br Med Bull. 2007;81–82:149–65. - PubMed
-
- Del Amo J, Malin AS, Pozniak A, De Cock KM. Does tuberculosis accelerate the progression of HIV disease? Evidence from basic science and epidemiology. Aids. 1999;13:1151–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
