

Multimorbidity patterns in the elderly: a new approach of disease clustering identifies complex interrelations between chronic conditions
- PMID: 21209965
- PMCID: PMC3012106
- DOI: 10.1371/journal.pone.0015941
Multimorbidity patterns in the elderly: a new approach of disease clustering identifies complex interrelations between chronic conditions
Abstract
Objective: Multimorbidity is a common problem in the elderly that is significantly associated with higher mortality, increased disability and functional decline. Information about interactions of chronic diseases can help to facilitate diagnosis, amend prevention and enhance the patients' quality of life. The aim of this study was to increase the knowledge of specific processes of multimorbidity in an unselected elderly population by identifying patterns of statistically significantly associated comorbidity.
Methods: Multimorbidity patterns were identified by exploratory tetrachoric factor analysis based on claims data of 63,104 males and 86,176 females in the age group 65+. Analyses were based on 46 diagnosis groups incorporating all ICD-10 diagnoses of chronic diseases with a prevalence ≥ 1%. Both genders were analyzed separately. Persons were assigned to multimorbidity patterns if they had at least three diagnosis groups with a factor loading of 0.25 on the corresponding pattern.
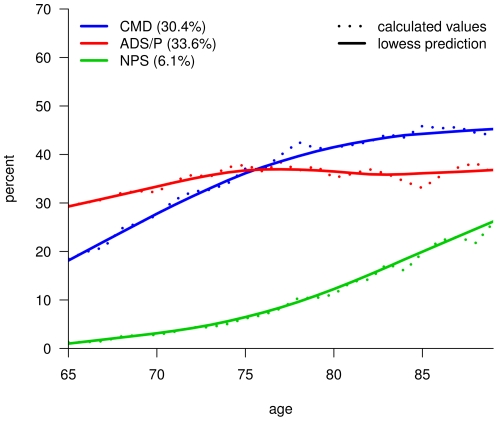
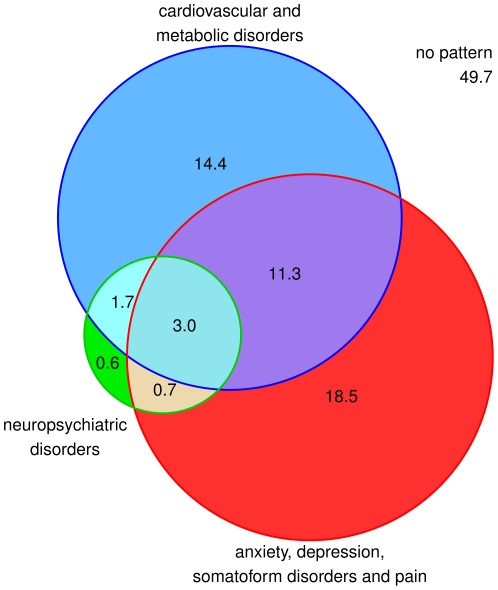
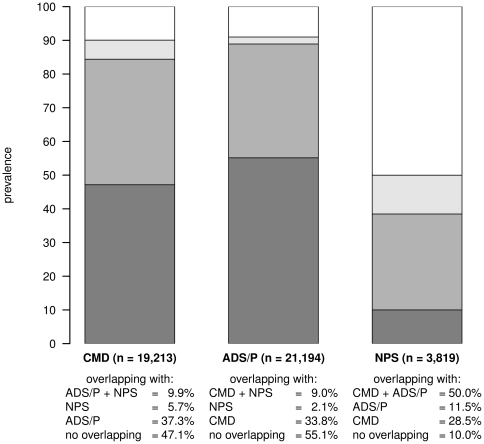
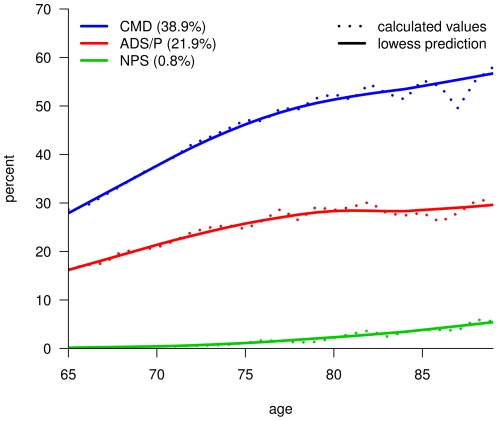
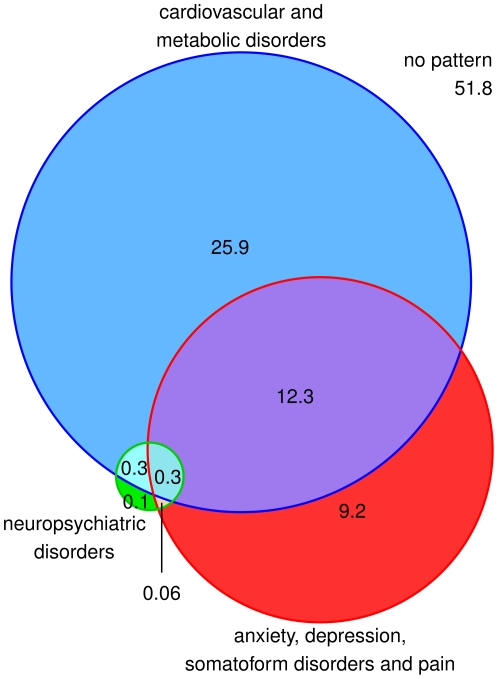
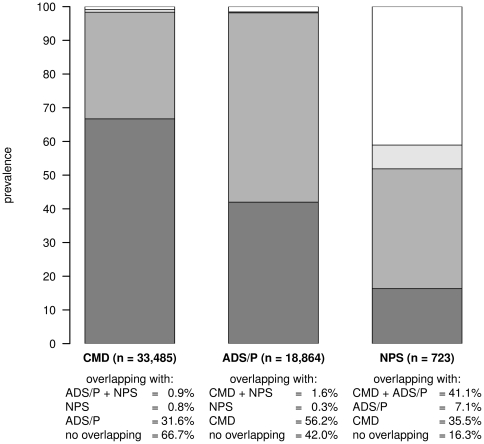
Results: Three multimorbidity patterns were found: 1) cardiovascular/metabolic disorders [prevalence female: 30%; male: 39%], 2) anxiety/depression/somatoform disorders and pain [34%; 22%], and 3) neuropsychiatric disorders [6%; 0.8%]. The sampling adequacy was meritorious (Kaiser-Meyer-Olkin measure: 0.85 and 0.84, respectively) and the factors explained a large part of the variance (cumulative percent: 78% and 75%, respectively). The patterns were largely age-dependent and overlapped in a sizeable part of the population. Altogether 50% of female and 48% of male persons were assigned to at least one of the three multimorbidity patterns.
Conclusion: This study shows that statistically significant co-occurrence of chronic diseases can be subsumed in three prevalent multimorbidity patterns if accounting for the fact that different multimorbidity patterns share some diagnosis groups, influence each other and overlap in a large part of the population. In recognizing the full complexity of multimorbidity we might improve our ability to predict needs and achieve possible benefits for elderly patients who suffer from multimorbidity.
Conflict of interest statement
Figures
References
-
- Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med. 2002;162:2269–2276. - PubMed
-
- Gijsen R, Hoeymans N, Schellevis FG, Ruwaard D, Satariano WA, et al. Causes and consequences of comorbidity: A review. J Clin Epidemiol. 2001;54:661–674. - PubMed
-
- Boyd CM, Darer J, Boult C, Fried LP, Boult L, et al. Clinical Practice Guidelines and Quality of Care for Older Patients with Multiple Comorbid Diseases. JAMA. 2005;294:716–724. - PubMed
-
- Schellevis FG. Comorbidity and Quality of Care. Utrecht: Drukkerij Pascal; 1993. Chronic Disease in General Practice.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
