

An updated study-level meta-analysis of randomised controlled trials on proning in ARDS and acute lung injury
- PMID: 21211010
- PMCID: PMC3222033
- DOI: 10.1186/cc9403
An updated study-level meta-analysis of randomised controlled trials on proning in ARDS and acute lung injury
Abstract
Introduction: In patients with acute lung injury (ALI) and/or acute respiratory distress syndrome (ARDS), recent randomised controlled trials (RCTs) showed a consistent trend of mortality reduction with prone ventilation. We updated a meta-analysis on this topic.
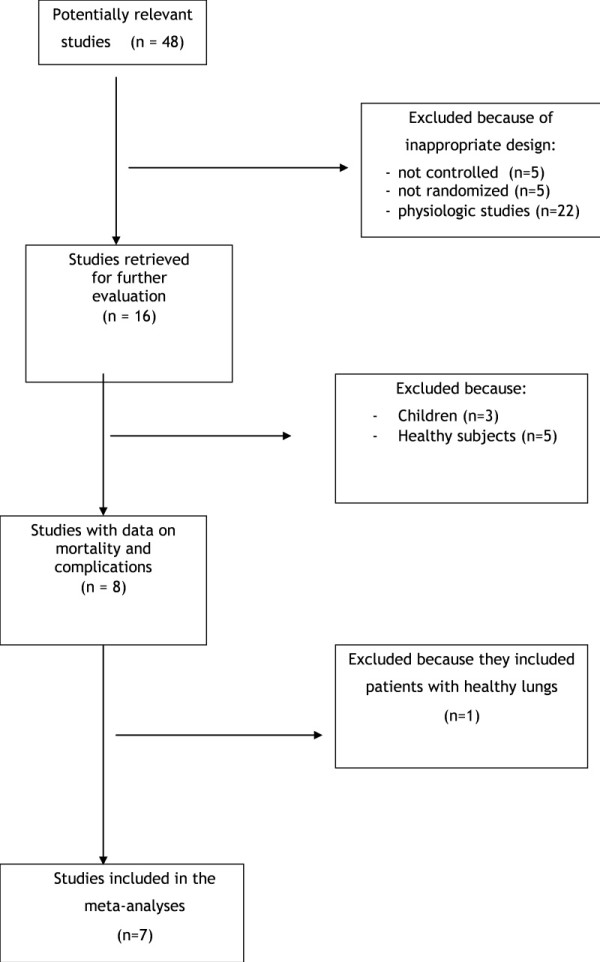
Methods: RCTs that compared ventilation of adult patients with ALI/ARDS in prone versus supine position were included in this study-level meta-analysis. Analysis was made by a random-effects model. The effect size on intensive care unit (ICU) mortality was computed in the overall included studies and in two subgroups of studies: those that included all ALI or hypoxemic patients, and those that restricted inclusion to only ARDS patients. A relationship between studies' effect size and daily prone duration was sought with meta-regression. We also computed the effects of prone positioning on major adverse airway complications.
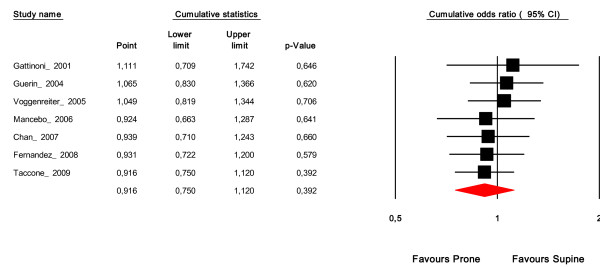
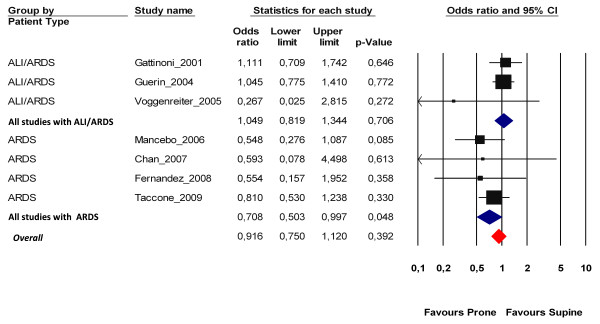
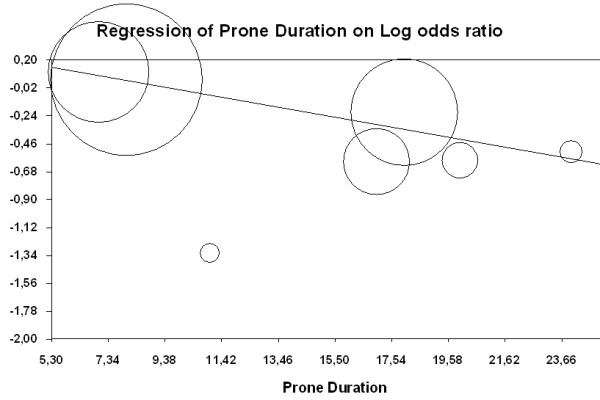
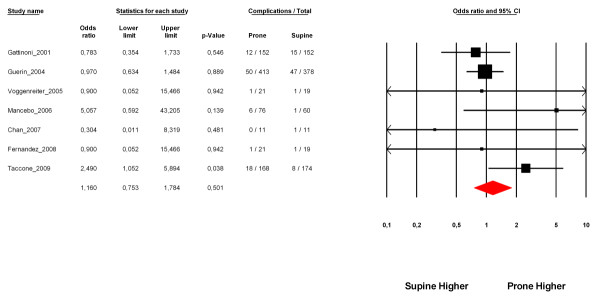
Results: Seven RCTs (including 1,675 adult patients, of whom 862 were ventilated in the prone position) were included. The four most recent trials included only ARDS patients, and also applied the longest proning durations and used lung-protective ventilation. The effects of prone positioning differed according to the type of study. Overall, prone ventilation did not reduce ICU mortality (odds ratio = 0.91, 95% confidence interval = 0.75 to 1.2; P = 0.39), but it significantly reduced the ICU mortality in the four recent studies that enrolled only patients with ARDS (odds ratio = 0.71; 95% confidence interval = 0.5 to 0.99; P = 0.048; number needed to treat = 11). Meta-regression on all studies disclosed only a trend to explain effect variation by prone duration (P = 0.06). Prone positioning was not associated with a statistical increase in major airway complications.
Conclusions: Long duration of ventilation in prone position significantly reduces ICU mortality when only ARDS patients are considered.
Figures
References
-
- Gattinoni L, Tognoni G, Pesenti A, Taccone P, Mascheroni D, Labarta V, Malacrida R, Di Giulio P, Fumagalli R, Pelosi P, Brazzi L, Latini R. Effect of prone positioning on the survival of patients with acute respiratory failure. N Engl J Med. 2001;345:568–573. doi: 10.1056/NEJMoa010043. - DOI - PubMed
-
- Guerin C, Gaillard S, Lemasson S, Ayzac L, Girard R, Beuret P, Palmier B, Le QV, Sirodot M, Rosselli S, Cadiergue V, Sainty JM, Barbe P, Combourieu E, Debatty D, Rouffineau J, Ezingeard E, Millet O, Guelon D, Rodriguez L, Martin O, Renault A, Sibille JP, Kaidomar M. Effects of systematic prone positioning in hypoxemic acute respiratory failure: a randomized controlled trial. JAMA. 2004;292:2379–2387. doi: 10.1001/jama.292.19.2379. - DOI - PubMed
-
- Voggenreiter G, Aufmkolk M, Stiletto RJ, Baacke MG, Waydhas C, Ose C, Bock E, Gotzen L, Obertacke U, Nast-Kolb D. Prone positioning improves oxygenation in post-traumatic lung injury - a prospective randomized trial. J Trauma. 2005;59:333–341. doi: 10.1097/01.ta.0000179952.95921.49. discussion 341-343. - DOI - PubMed
-
- Curley MA, Hibberd PL, Fineman LD, Wypij D, Shih MC, Thompson JE, Grant MJ, Barr FE, Cvijanovich NZ, Sorce L, Luckett PM, Matthay MA, Arnold JH. Effect of prone positioning on clinical outcomes in children with acute lung injury: a randomized controlled trial. JAMA. 2005;294:229–237. doi: 10.1001/jama.294.2.229. - DOI - PMC - PubMed
-
- Abroug F, Ouanes-Besbes L, Elatrous S, Brochard L. The effect of prone positioning in acute respiratory distress syndrome or acute lung injury: a meta-analysis. Areas of uncertainty and recommendations for research. Intensive Care Med. 2008;34:1002–1011. doi: 10.1007/s00134-008-1062-3. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
