

Addressing institutional amplifiers in the dynamics and control of tuberculosis epidemics
- PMID: 21212197
- PMCID: PMC3005502
- DOI: 10.4269/ajtmh.2011.10-0472
Addressing institutional amplifiers in the dynamics and control of tuberculosis epidemics
Abstract
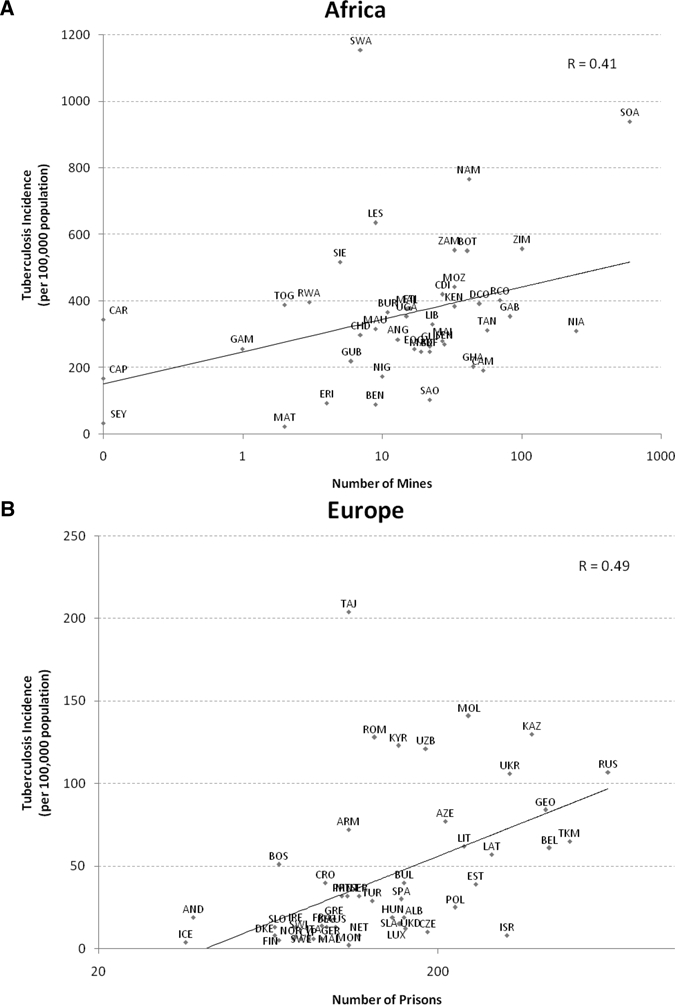
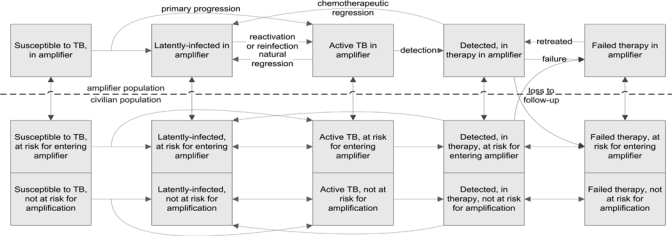
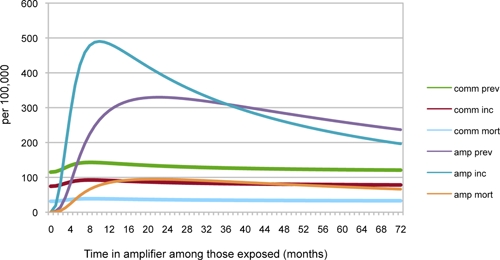
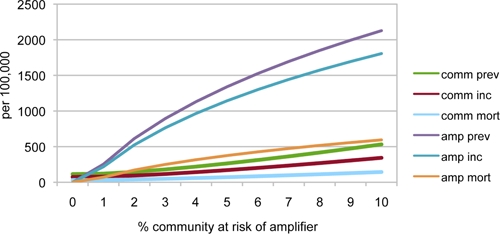
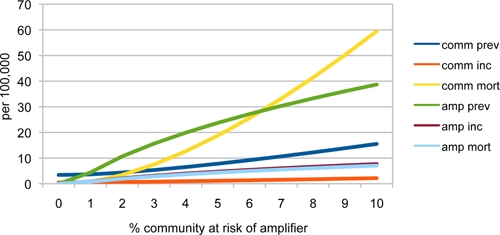
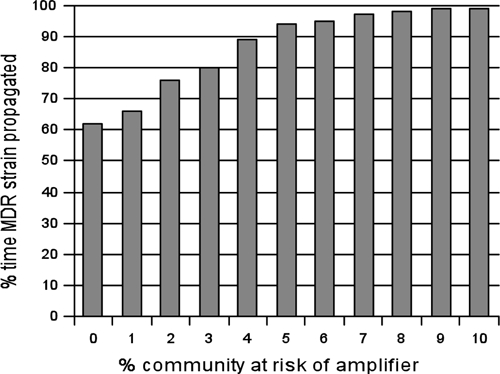
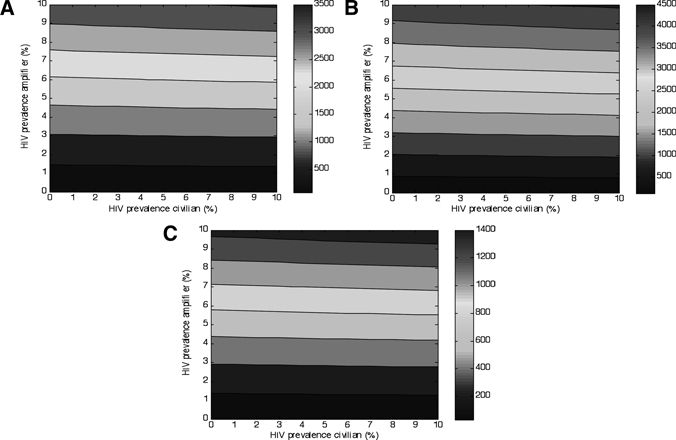
Tuberculosis outbreaks originating in prisons, mines, or hospital wards can spread to the larger community. Recent proposals have targeted these high-transmission institutional amplifiers by improving case detection, treatment, or reducing the size of the exposed population. However, what effects these alternative proposals may have is unclear. We mathematically modeled these control strategies and found case detection and treatment methods insufficient in addressing epidemics involving common types of institutional amplifiers. Movement of persons in and out of amplifiers fundamentally altered the transmission dynamics of tuberculosis in a manner not effectively mitigated by detection or treatment alone. Policies increasing the population size exposed to amplifiers or the per-person duration of exposure within amplifiers potentially worsened incidence, even in settings with high rates of detection and treatment success. However, reducing the total population size entering institutional amplifiers significantly lowered tuberculosis incidence and the risk of propagating new drug-resistant tuberculosis strains.
Figures
References
-
- World Health Organization . Global Tuberculosis Control: Epidemiology, Strategy, Financing. Geneva: World Health Organization. WHO/HTM/TB/2009.411; 2009.
-
- Dorman SE, Chaisson RE. From magic bullets back to the Magic Mountain: the rise of extensively drug-resistant tuberculosis. Nat Med. 2007;13:295–298. - PubMed
-
- Gandhi NR, Moll A, Sturm AW, Pawinski R, Govender T, Lalloo U, Zeller K, Andrews J, Friedland G. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet. 2006;368:1575–1580. - PubMed
-
- World Health Organization . Global Tuberculosis Control: Surveillance, Planning, Financing. Geneva: World Health Organization. WHO/HTM/TB2008.393; 2008.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
