

Systematic review of medical treatment in melanoma: current status and future prospects
- PMID: 21212434
- PMCID: PMC3228046
- DOI: 10.1634/theoncologist.2010-0190
Systematic review of medical treatment in melanoma: current status and future prospects
Abstract
The incidence of melanoma is increasing worldwide, and the prognosis for patients with high-risk or advanced metastatic melanoma remains poor despite advances in the field. Standard treatment for patients with thick (≥2.0 mm) primary melanoma with or without regional metastases to lymph nodes is surgery followed by adjuvant therapy or clinical trial enrollment. Adjuvant therapy with interferon-α and cancer vaccines is discussed in detail. Patients who progress to stage IV metastatic melanoma have a median survival of ≤1 year. Standard treatment with chemotherapy yields low response rates, of which few are durable. Cytokine therapy with IL-2 achieves durable benefits in a greater fraction, but it is accompanied by severe toxicities that require the patient to be hospitalized for support during treatment. A systematic literature review of treatments for advanced, metastatic disease was conducted to present the success of current treatments and the promise of those still in clinical development that may yield incremental improvements in the treatment of advanced, metastatic melanoma.
Conflict of interest statement
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the independent peer reviewers.
Figures
References
-
- Lens MB, Dawes M. Global perspectives of contemporary epidemiological trends of cutaneous malignant melanoma. Br J Dermatol. 2004;150:179–185. - PubMed
-
- Molife R, Hancock BW. Adjuvant therapy of malignant melanoma. Crit Rev Oncol Hematol. 2002;44:81–102. - PubMed
-
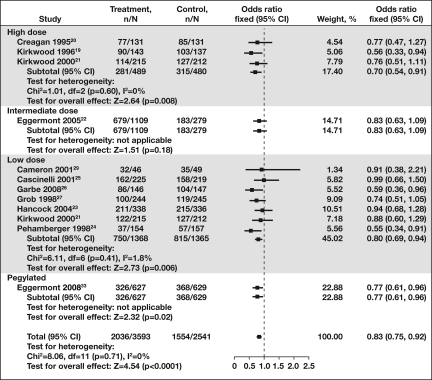
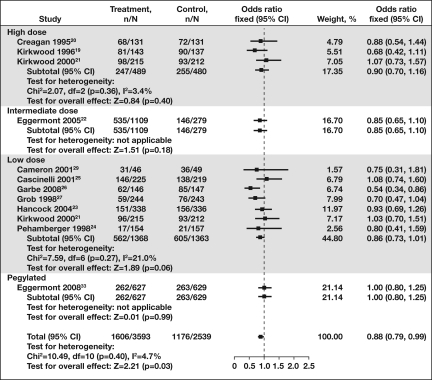
- Wheatley K, Ives N, Hancock B, et al. Does adjuvant interferon-alpha for high-risk melanoma provide a worthwhile benefit? A meta-analysis of the randomised trials. Cancer Treat Rev. 2003;29:241–252. - PubMed
-
- Mocellin S, Pasquali S, Rossi CR, et al. Interferon alpha adjuvant therapy in patients with high-risk melanoma: a systematic review and meta-analysis. J Natl Cancer Inst. 2010;102:493–501. - PubMed
-
- Eggermont AM, Kirkwood JM. Re-evaluating the role of dacarbazine in metastatic melanoma: what have we learned in 30 years? Eur J Cancer. 2004;40:1825–1836. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
