

PIK3CA mutations in patients with advanced cancers treated with PI3K/AKT/mTOR axis inhibitors
- PMID: 21216929
- PMCID: PMC3072168
- DOI: 10.1158/1535-7163.MCT-10-0994
PIK3CA mutations in patients with advanced cancers treated with PI3K/AKT/mTOR axis inhibitors
Abstract
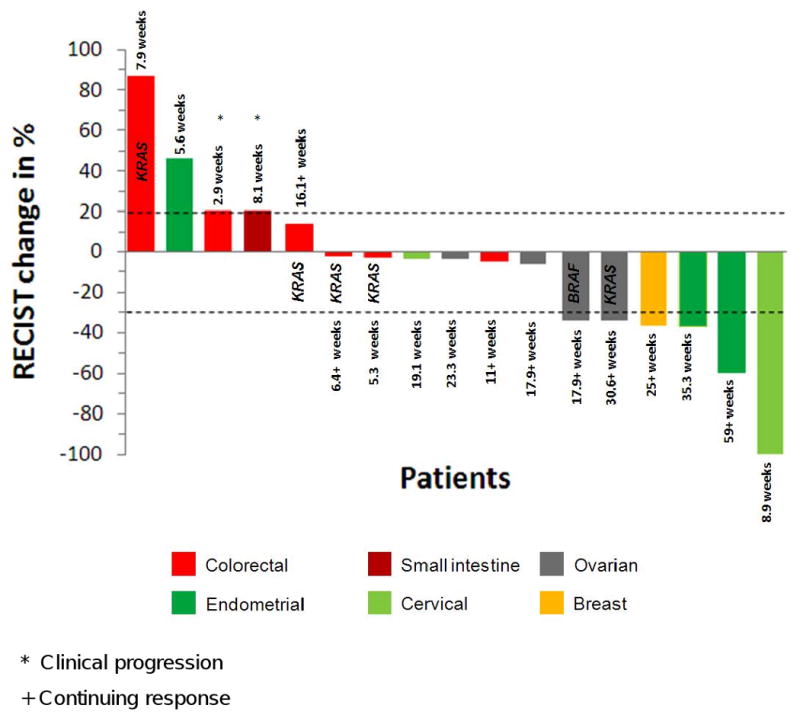
Preclinical data suggest that PIK3CA mutations predict response to PI3K/AKT/mTOR inhibitors. Concomitant KRAS or BRAF mutations may mediate resistance. Therefore, tumors from patients referred to the phase I program for targeted therapy starting in October 2008 were analyzed for PIK3CA mutations using PCR-based DNA sequencing of exons 9 and 20. Consecutive patients with diverse tumor types and PIK3CA mutation were treated whenever possible with agents targeting the PI3K/AKT/mTOR pathway. Overall, PIK3CA mutations were detected in 25 of 217 patients (11.5%; exon 9, n = 11; exon 20, n = 14). In tumor types with more than 10 patients tested, PIK3CA mutations were most frequent in endometrial (3 of 14, 21%), ovarian (5 of 30, 17%), colorectal (9 of 54, 17%), breast (2 of 14, 14%), cervical (2 of 15, 13%), and squamous cell cancer of the head and neck (1 of 11, 9%). Of the 25 patients with PIK3CA mutations, 17 (68%) were treated on a protocol that included a PI3K/AKT/mTOR pathway inhibitor, and 6 (35%) achieved a partial response. In contrast, only 15 of 241 patients (6%) without documented PIK3CA mutations treated on the same protocols responded (P = 0.001). Of the 17 patients with PIK3CA mutations, 6 (35%) had simultaneous KRAS or BRAF mutations (colorectal, n = 4; ovarian, n = 2). Colorectal cancer patients with PIK3CA and KRAS mutations did not respond to therapy, whereas both ovarian cancer patients with PIK3CA and KRAS or BRAF mutations did. In conclusion, PIK3CA mutations were detected in 11.5% of patients with diverse solid tumors. The response rate was significantly higher for patients with PIK3CA mutations treated with PI3K/AKT/mTOR pathway inhibitors than for those without documented mutations.
©2011 AACR.
Conflict of interest statement
Figures
Comment in
-
Research highlights. PI3K/AKT/mTOR inhibitors would require PI3KCA-mutation analysis.Pharmacogenomics. 2011 Oct;12(10):1382. Pharmacogenomics. 2011. PMID: 22121542 No abstract available.
References
-
- Druker BJ, Talpaz M, Resta DJ, et al. Efficacy and safety of a specific inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. N Engl J Med. 2001 Apr 5;344(14):1031–7. - PubMed
-
- Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med. 2002 Aug 15;347(7):472–80. - PubMed
-
- Braiteh F, Kurzrock R. Uncommon tumors and exceptional therapies: paradox or paradigm? Mol Cancer Ther. 2007 Apr;6(4):1175–9. - PubMed
-
- Stewart DJ, Kurzrock R. Cancer: the road to Amiens. J Clin Oncol. 2009 Jan 20;27(3):328–33. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
