

Aspirin-exacerbated respiratory disease: evaluation and management
- PMID: 21217919
- PMCID: PMC3005316
- DOI: 10.4168/aair.2011.3.1.3
Aspirin-exacerbated respiratory disease: evaluation and management
Abstract
The clinical syndrome of aspirin-exacerbated respiratory disease (AERD) is a condition where inhibition of cyclooxygenase-1 (COX-1) induces attacks of upper and lower airway reactions, including rhinorrhea and varying degrees of bronchospasm and laryngospasm. Although the reaction is not IgE-mediated, patients can also present with anaphylactic hypersensitivity reactions, including hypotension, after exposure to COX-1 inhibiting drugs. All patients with AERD have underlying nasal polyps and intractable sinus disease which may be difficult to treat with standard medical and surgical interventions. This review article focuses on the management of AERD patients with a particular emphasis on aspirin desensitization and continuous treatment with aspirin.
Keywords: Aspirin-exacerbated respiratory disease; Samter's triad; aspirin desensitization; aspirin sensitivity; asthma; chronic sinusitis; nasal polyps.
Conflict of interest statement
The views expressed in this article are those of the author(s) and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense or the United States Government.
There are no financial or other issues that might lead to conflict of interest.
Figures
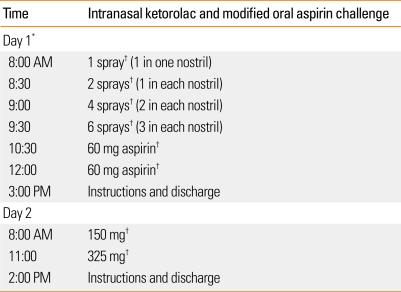
Take ketorolac tromethamine (60 mg/2 mL) and preservative free normal saline (2.75 mL).
Mix in an emptied Nasocort AQ® spray bottle.
Prime with 5 sprays before use, then each spray actuates 1.26 mg of solution.
Instruct patient and medical personnel to tilt head down while spraying and sniff gently to avoid swallowing solution.
- Naso-ocular alone
- Naso-ocular and a 15% or more decline in FEV1 (Classic reaction)
- Lower respiratory reaction only (FEV1 declines by >20%)
- Laryngospasm with or without a, b, c (flat or notched inspiratory curve)
- Systemic reaction: hives, flush, gastric pain, hypotension
After a reaction has been treated and resolved, repeat provoking dose.
If no reaction, continue to escalate the doses as above.
At 325 mg of aspirin, desensitization is always completed.
References
-
- Szczeklik A, Nizankowska-Mogilnicka E, Sanak M. Hypersensitivity to aspirin and non-steroidal anti-inflammatory drugs. In: Adkinson NF Jr, Bochner BS, Busse WW, Holgate ST, Lemanske RF Jr, Simons FER, editors. Middleton's allergy: principles and practice. 7th ed. New York: Mosby; 2009. pp. 1227–1240.
-
- Stevenson DD. Aspirin sensitivity and desensitization for asthma and sinusitis. Curr Allergy Asthma Rep. 2009;9:155–163. - PubMed
-
- McDonald JR, Mathison DA, Stevenson DD. Aspirin intolerance in asthma. Detection by oral challenge. J Allergy Clin Immunol. 1972;50:198–207. - PubMed
-
- Weber RW, Hoffman M, Raine DA, Jr, Nelson HS. Incidence of bronchoconstriction due to aspirin, azo dyes, non-azo dyes, and preservatives in a population of perennial asthmatics. J Allergy Clin Immunol. 1979;64:32–37. - PubMed
