

Severe venous neointimal hyperplasia prior to dialysis access surgery
- PMID: 21220751
- PMCID: PMC3145379
- DOI: 10.1093/ndt/gfq733
Severe venous neointimal hyperplasia prior to dialysis access surgery
Abstract
Background: Venous neointimal hyperplasia is the most common cause of arteriovenous (AV) fistula and graft dysfunction following dialysis access surgery. However, the pathogenetic impact of pre-existing venous neointimal hyperplasia at the time of AV access creation on final clinical success is currently unknown in the setting of advanced chronic kidney disease (CKD) and end-stage renal disease (ESRD) patients. The aim of this study was to perform a detailed histological, morphometric, and immunohistochemical analysis of vein specimens in advanced CKD and ESRD patients collected at the time of new vascular access placement.
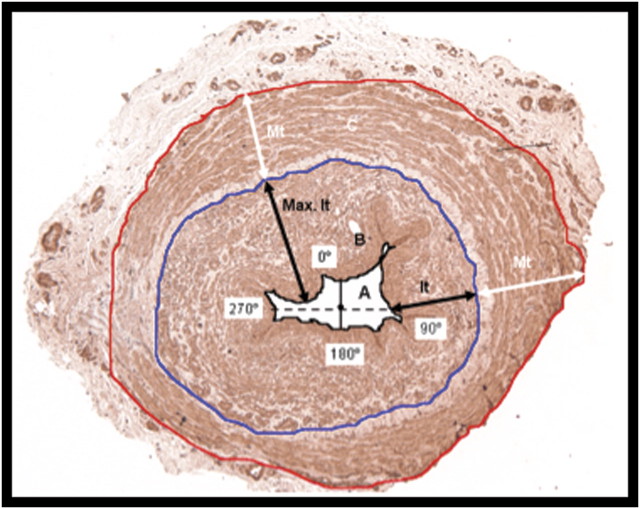
Methods: Vein samples from 12 patients were collected at the time of AV access creation near the site of AV anastomosis. Histological, immunohistochemistry and morphometric studies were performed on these vein samples.
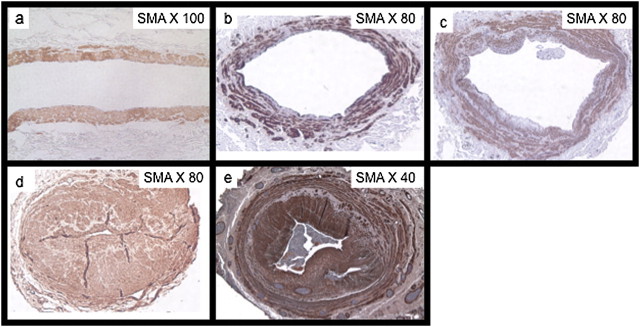
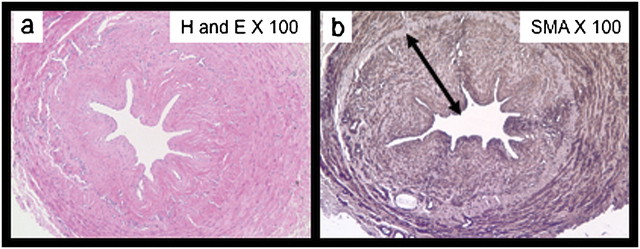
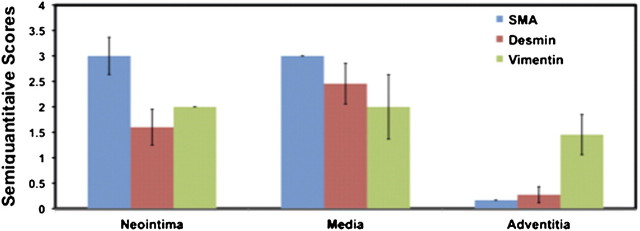
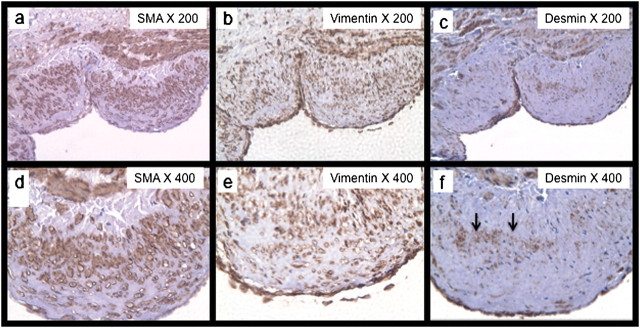
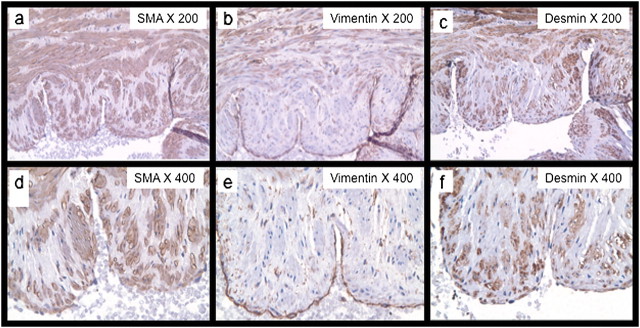
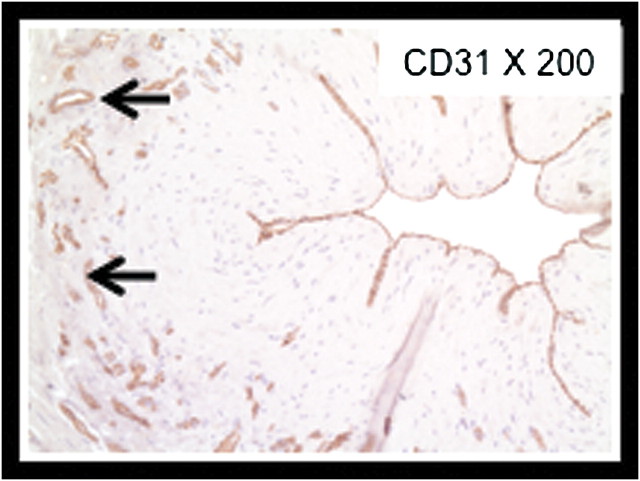
Results: Examination of the tissue specimens obtained at the time of surgery showed neointimal hyperplasia in 10 of 12 specimens, ranging from minimal to very severe. The majority of cells within the neointima were myofibroblasts with a minority of contractile smooth muscle cells present.
Conclusion: Our work represents a detailed description of the morphometric and cellular phenotypic lesions present in the veins of CKD and ESRD patients, prior to dialysis access placement. These studies (i) suggest the future possibility of a new predictive marker (pre-existing venous neointimal hyperplasia) for AV dialysis access dysfunction and (ii) open the door for the future development of novel local therapies for optimization of the venous substrate on which the dialysis access is created.
Figures
References
-
- Roy-Chaudhury P, Sukhatme VP, Cheung AK. Hemodialysis vascular access dysfunction: a cellular and molecular viewpoint. J Am Soc Nephrol. 2006;17:1112–1127. - PubMed
-
- Roy-Chaudhury P, Lee TC. Vascular stenosis: biology and interventions. Curr Opin Nephrol Hypertens. 2007;16:516–522. - PubMed
-
- Allan JC, Bertram K, Charles H, et al. United States Renal Data System 2006 Annual Data Report Abstract. Am J Kidney Dis. 2006;49:A6–A7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
