

T cell activation and senescence predict subclinical carotid artery disease in HIV-infected women
- PMID: 21220772
- PMCID: PMC3071219
- DOI: 10.1093/infdis/jiq071
T cell activation and senescence predict subclinical carotid artery disease in HIV-infected women
Abstract
Background: Individuals infected with human immunodeficiency virus (HIV) have increased risk of cardiovascular events. It is unknown whether T cell activation and senescence, 2 immunologic sequelae of HIV infection, are associated with vascular disease among HIV-infected adults.
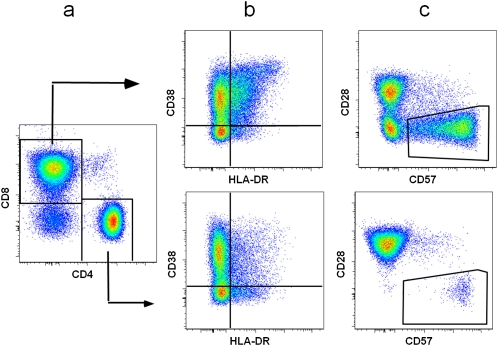
Methods: T cell phenotyping and carotid ultrasound were assessed among 115 HIV-infected women and 43 age- and race/ethnicity-matched HIV-uninfected controls participating in the Women's Interagency HIV Study. Multivariate analyses were used to assess the association of T cell activation (CD38(+)HLA-DR(+)) and senescence (CD28(-)CD57(+)) with subclinical carotid artery disease.
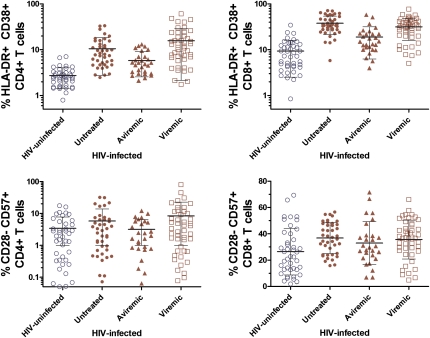
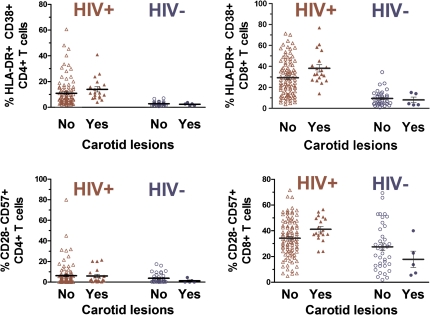
Results: Compared with HIV-uninfected women, frequencies of CD4(+)CD38(+)HLA-DR(+), CD8(+)CD38(+)HLA-DR(+), and CD8(+)CD28(-)CD57(+) T cells were higher among HIV-infected women, including those who achieved viral suppression while receiving antiretroviral treatment. Among HIV-infected women, adjusted for age, antiretroviral medications, and viral load, higher frequencies of activated CD4(+) and CD8(+) T cells and immunosenescent CD8(+) T cells were associated with increased prevalence of carotid artery lesions (prevalence ratio(lesions) associated with activated CD4(+) T cells, 1.6 per SD [95% confidence interval {CI}, 1.1-2.2]; P = .02; prevalence ratio(lesions) associated with activated CD8(+) T cells, 2.0 per SD [95% CI, 1.2-3.3]; P < .01; prevalence ratio(lesions) associated with senescent CD8(+) T cells, 1.9 per SD [95% CI, 1.1-3.1]; P = .01).
Conclusions: HIV-associated T cell changes are associated with subclinical carotid artery abnormalities, which may be observed even among those patients achieving viral suppression with effective antiretroviral therapy.
Figures
Comment in
-
Immune dysregulation and vascular risk in HIV-infected patients: implications for clinical care.J Infect Dis. 2011 Feb 15;203(4):439-41. doi: 10.1093/infdis/jiq084. Epub 2011 Jan 10. J Infect Dis. 2011. PMID: 21220778 Free PMC article. No abstract available.
References
-
- Currier JS, Taylor A, Boyd F, Dezii CM, Kawabata H, Burtcel B, et al. Coronary heart disease in HIV-infected individuals. J Acquir Immune Defic Syndr. 2003;33:506–12. - PubMed
-
- Bonnet D, Aggoun Y, Szezepanski I, Bellal N, Blanche S. Arterial stiffness endothelial dysfunction in HIV-infected children. AIDS. 2004;18:1037–41. - PubMed
-
- El-Sadr WM, Lundgren JD, Neaton JD, Gordin F, Abrams D, Arduino RC, et al. CD4+ count-guided interruption of antiretroviral treatment. N Engl J Med. 2006;355:2283–96. - PubMed
-
- Mary-Krause M, Cotte L, Simon A, Partisani M, Costagliola D. Increased risk of myocardial infarction with duration of protease inhibitor therapy in HIV-infected men. AIDS. 2003;17:2479–86. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UO1-AI-34989/AI/NIAID NIH HHS/United States
- P30AI027763/AI/NIAID NIH HHS/United States
- UO1-AI-35004/AI/NIAID NIH HHS/United States
- UO1-AI-34993/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- UO1-AI-42590/AI/NIAID NIH HHS/United States
- UO1-AI-31834/AI/NIAID NIH HHS/United States
- 1R01HL083760/HL/NHLBI NIH HHS/United States
- UO1-HD-32632/HD/NICHD NIH HHS/United States
- UO1-AI-34994/AI/NIAID NIH HHS/United States
- 1R01HL095140/HL/NHLBI NIH HHS/United States
