

Comparison of the prognostic and predictive utilities of the 21-gene Recurrence Score assay and Adjuvant! for women with node-negative, ER-positive breast cancer: results from NSABP B-14 and NSABP B-20
- PMID: 21221771
- PMCID: PMC4266581
- DOI: 10.1007/s10549-010-1331-z
Comparison of the prognostic and predictive utilities of the 21-gene Recurrence Score assay and Adjuvant! for women with node-negative, ER-positive breast cancer: results from NSABP B-14 and NSABP B-20
Abstract
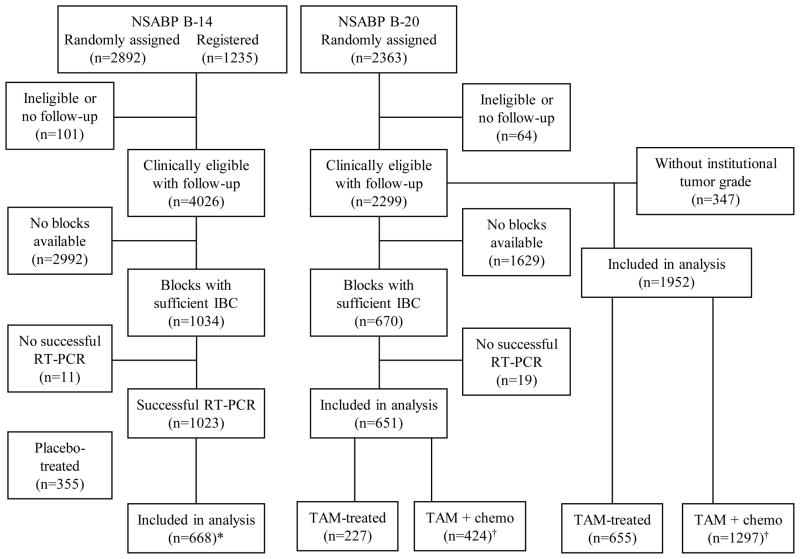
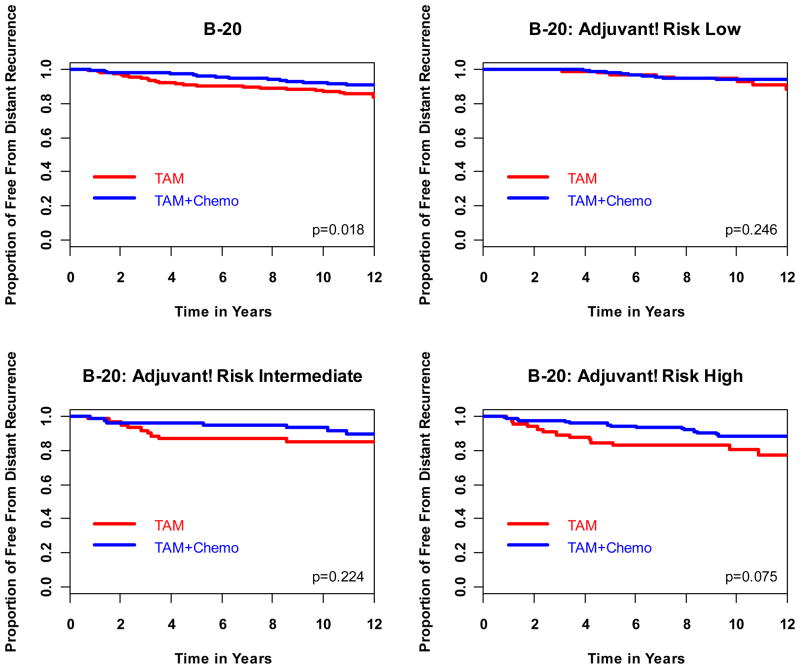
The Oncotype DX Recurrence Score (RS) is a validated genomic predictor of outcome and response to adjuvant chemotherapy in ER-positive breast cancer. Adjuvant! was developed using SEER registry data and results from the Early Breast Cancer Clinical Trialists' overview analyses to estimate outcome and benefit from adjuvant hormonal therapy and chemotherapy. In this report we compare the prognostic and predictive utility of these two tools in node-negative, ER-positive breast cancer. RS and Adjuvant! results were available from 668 tamoxifen-treated NSABP B-14 patients, 227 tamoxifen-treated NSABP B-20 patients, and 424 chemotherapy plus tamoxifen-treated B-20 patients. Adjuvant! results were also available from 1952 B-20 patients. The primary endpoint was distant recurrence-free interval (DRFI). Cox proportional hazards models were used to compare the prognostic and predictive utility of RS and Adjuvant!. Both RS (P < 0.001) and Adjuvant! (P = 0.002) provided strong independent prognostic information in tamoxifen-treated patients. Combining RS and individual clinicopathologic characteristics provided greater prognostic discrimination than combining RS and the composite Adjuvant!. In the B-20 cohort with RS results (n = 651), RS was significantly predictive of chemotherapy benefit (interaction P = 0.031 for DRFI, P = 0.011 for overall survival [OS], P = 0.082 for disease-free survival [DFS]), but Adjuvant! was not (interaction P = 0.99, P = 0.311, and P = 0.357, respectively). However, in the larger B-20 sub-cohort (n = 1952), Adjuvant! was significantly predictive of chemotherapy benefit for OS (interaction P = 0.009) but not for DRFI (P = 0.219) or DFS (P = 0.099). Prognostic estimates can be optimized by combining RS and clinicopathologic information instead of simply combining RS and Adjuvant!. RS should be used for estimating relative chemotherapy benefit.
Conflict of interest statement
Even though the NSABP Statistical Center has received research funding from Genomic Health, this study was not supported by Genomic Health. SS is a full-time employee and a stockholder in Genomic Health. GT, SJA, and JPC declare no potential conflicts of interest. EPM has been a consultant and on the speaker’s bureau of Genomic Health. There are no other potential conflicts of interest reported.
Figures



References
-
- Van De Vijver M, He YD, Van’t Veer LJ, et al. A Gene-Expression Signature as a Predictor of Survival in Breast Cancer. N Engl J Med. 2002;347:1999–2009. - PubMed
-
- Van 't Veer LJ, Dai H, van de Vijver MJ, et al. Gene expression profiling predicts clinical outcome of breast cancer. Nature. 2002;415:530–536. - PubMed
-
- Foekens JA, Atkins D, Zhang Y, et al. Multicenter Validation of a Gene Expression-Based Prognostic Signature in Lymph Node-Negative Primary Breast Cancer. J Clin Oncol. 2006;24:1665–1671. - PubMed
-
- Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351:2817–26. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
