

The effects of latent variables in the development of comorbidity among common mental disorders
- PMID: 21225850
- PMCID: PMC3228602
- DOI: 10.1002/da.20760
The effects of latent variables in the development of comorbidity among common mental disorders
Abstract
Background: Although numerous studies have examined the role of latent predispositions to internalizing and externalizing disorders in the structure of comorbidity among common mental disorders, none examined latent predispositions in predicting development of comorbidity.
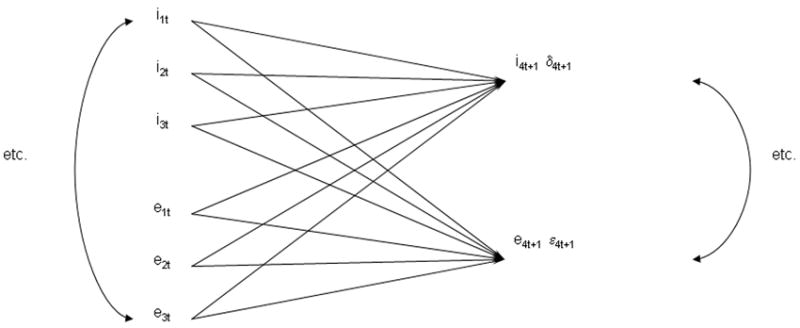
Methods: A novel method was used to study the role of latent variables in the development of comorbidity among lifetime DSM-IV disorders in the National Comorbidity Surveys. Broad preliminary findings are briefly presented to describe the method. The method used survival analysis to estimate time-lagged associations among 18 lifetime DSM-IV anxiety, mood, behavior, and substance disorders. A novel estimation approach examined the extent to which these predictive associations could be explained by latent canonical variables representing internalizing and externalizing disorders.
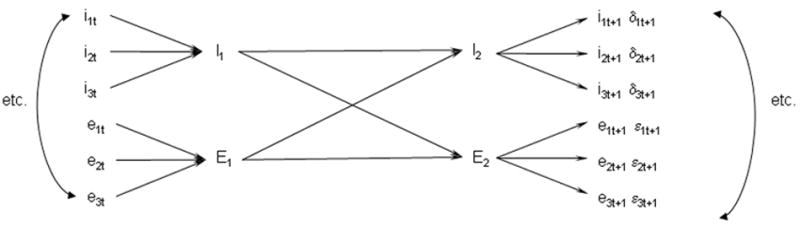
Results: Consistently significant positive associations were found between temporally primary and secondary disorders. Within-domain time-lagged associations were generally stronger than between-domain associations. The vast majority of associations were explained by a model that assumed mediating effects of latent internalizing and externalizing variables, although the complexity of this model differed across samples. A number of intriguing residual associations emerged that warrant further investigation.
Conclusions: The good fit of the canonical model suggests that common causal pathways account for most comorbidity among the disorders considered. These common pathways should be the focus of future research on the development of comorbidity. However, the existence of several important residual associations shows that more is involved than simple mediation. The method developed to carry out these analyses provides a unique way to pinpoint these significant residual associations for subsequent focused study.
Depression and Anxiety, 2011. © 2011 Wiley-Liss, Inc.
Conflict of interest statement
Figures
References
-
- Demyttenaere K, Bruffaerts R, Posada-Villa J, et al. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization World Mental Health surveys. JAMA. 2004;291:2581–2590. - PubMed
-
- Krueger RF. The structure of common mental disorders. Arch Gen Psychiatry. 1999;56:921–926. - PubMed
-
- Cox BJ, Swinson RP. Instrument to assess depersonalization-derealization in panic disorder. Depress Anxiety. 2002;15:172–175. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 DA016558/DA/NIDA NIH HHS/United States
- R01 MH066627/MH/NIMH NIH HHS/United States
- R01 MH046376/MH/NIMH NIH HHS/United States
- R01-DA016558/DA/NIDA NIH HHS/United States
- R01-MH069864/MH/NIMH NIH HHS/United States
- R13-MH066849/MH/NIMH NIH HHS/United States
- R01DA012058/DA/NIDA NIH HHS/United States
- R01 MH070884/MH/NIMH NIH HHS/United States
- U13 MH066849/MH/NIMH NIH HHS/United States
- R01 MH077883/MH/NIMH NIH HHS/United States
- R03 TW006481/TW/FIC NIH HHS/United States
- CAPMC/ CIHR/Canada
- R01 MH069864/MH/NIMH NIH HHS/United States
- R01MH070884/MH/NIMH NIH HHS/United States
- U01MH60220/MH/NIMH NIH HHS/United States
- U01MH060220-09S1/MH/NIMH NIH HHS/United States
- K05 DA015799/DA/NIDA NIH HHS/United States
- R03-TW006481/TW/FIC NIH HHS/United States
- U01 MH060220/MH/NIMH NIH HHS/United States
- R01-MH66627/MH/NIMH NIH HHS/United States
- R01-MH077883/MH/NIMH NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- R13 MH066849/MH/NIMH NIH HHS/United States
- R01 DA012058/DA/NIDA NIH HHS/United States
