

Review
doi: 10.1056/NEJMct1004810.
Iron-chelating therapy for transfusional iron overload
Affiliations
- PMID: 21226580
- PMCID: PMC3078566
- DOI: 10.1056/NEJMct1004810
Item in Clipboard
Review
Iron-chelating therapy for transfusional iron overload
N Engl J Med.
.
Abstract
A 16-year-old boy with sickle cell anemia undergoes routine screening with transcranial Doppler ultrasonography to assess the risk of stroke. This examination shows an abnormally elevated blood-flow velocity in the middle cerebral artery. The hemoglobin level is 7.2 g per deciliter, the reticulocyte count is 12.5%, and the fetal hemoglobin level is 8.0%. Long-term treatment with red-cell transfusion is initiated to prevent stroke. A hematologist recommends prophylactic iron-chelating therapy.
Figures
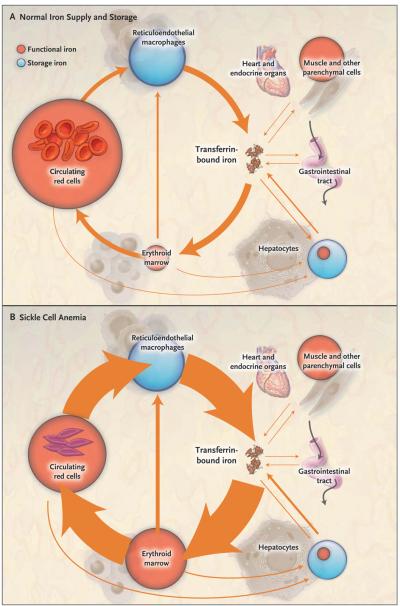
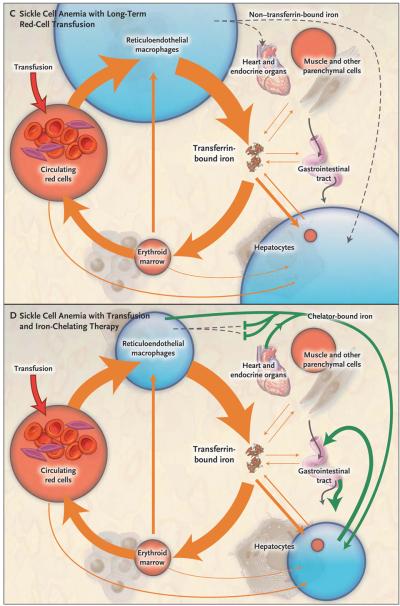
In all four panels, the area of the red and blue circles is roughly proportional to the amount of iron in each pool, and the width of the arrows is roughly proportional to the daily magnitude of the iron flux. Panel A shows normal iron supply and storage in a healthy person without sickle cell disease (i.e., with hemoglobin A). The major pathway of internal iron exchange is a unidirectional flow from plasma transferrin to the erythroid marrow to circulating red cells to reticuloendothelial macrophages and back to plasma transferrin (orange arrows). In the circulating plasma, virtually all iron is bound to transferrin. Panel B shows that in sickle cell anemia, hemolysis shortens the average life span of the red cell from about 4 months to 5 or 6 weeks, increasing red-cell catabolism by reticuloendothelial macrophages and increasing iron delivery to the erythroid marrow by 6 to 8 times the normal rate. There is little ineffective erythropoiesis, and iron absorption from the gastrointestinal tract is not increased. Panel C shows that long-term red-cell transfusion decreases erythroid marrow activity to 2 to 3 times the normal rate but results in accumulation of iron in reticuloendothelial macrophages and hepatocytes. Eventually, the capacity for safe storage is exceeded, with the appearance of plasma non–transferrin-bound iron (dashed arrow) and its progressive deposition in the heart and endocrine organs. In Panel D, the green arrows show that iron-chelating therapy with deferasirox can clear plasma non–transferrin-bound iron and remove excess iron from the liver, heart, and other organs, with subsequent excretion through the bile into the stool.
In all four panels, the area of the red and blue circles is roughly proportional to the amount of iron in each pool, and the width of the arrows is roughly proportional to the daily magnitude of the iron flux. Panel A shows normal iron supply and storage in a healthy person without sickle cell disease (i.e., with hemoglobin A). The major pathway of internal iron exchange is a unidirectional flow from plasma transferrin to the erythroid marrow to circulating red cells to reticuloendothelial macrophages and back to plasma transferrin (orange arrows). In the circulating plasma, virtually all iron is bound to transferrin. Panel B shows that in sickle cell anemia, hemolysis shortens the average life span of the red cell from about 4 months to 5 or 6 weeks, increasing red-cell catabolism by reticuloendothelial macrophages and increasing iron delivery to the erythroid marrow by 6 to 8 times the normal rate. There is little ineffective erythropoiesis, and iron absorption from the gastrointestinal tract is not increased. Panel C shows that long-term red-cell transfusion decreases erythroid marrow activity to 2 to 3 times the normal rate but results in accumulation of iron in reticuloendothelial macrophages and hepatocytes. Eventually, the capacity for safe storage is exceeded, with the appearance of plasma non–transferrin-bound iron (dashed arrow) and its progressive deposition in the heart and endocrine organs. In Panel D, the green arrows show that iron-chelating therapy with deferasirox can clear plasma non–transferrin-bound iron and remove excess iron from the liver, heart, and other organs, with subsequent excretion through the bile into the stool.
Comment in
-
Iron-chelating therapy for transfusional iron overload.N Engl J Med. 2011 Apr 14;364(15):1476-7; author reply 1477. doi: 10.1056/NEJMc1101838. N Engl J Med. 2011. PMID: 21488786 No abstract available.
-
Iron-chelating therapy for transfusional iron overload.N Engl J Med. 2011 Apr 14;364(15):1476; author reply 1477. doi: 10.1056/NEJMc1101838. N Engl J Med. 2011. PMID: 21488787 No abstract available.
-
Iron-chelating therapy for transfusional iron overload.N Engl J Med. 2011 Apr 14;364(15):1475-6; author reply 1477. doi: 10.1056/NEJMc1101838. N Engl J Med. 2011. PMID: 21488788 No abstract available.
References
-
- Adams RJ, McKie VC, Hsu L, et al. Prevention of a first stroke by transfusions in children with sickle cell anemia and abnormal results on transcranial Doppler ultrasonography. N Engl J Med. 1998;339:5–11. - PubMed
-
- Vichinsky EP, MacKlin EA, Waye JS, Lorey F, Olivieri NF. Changes in the epidemiology of thalassemia in North America: a new minority disease. Pediatrics. 2005;116(6):e818–e825. - PubMed
-
- Weatherall DJ, Clegg JB. The thalassemia syndromes. 4th ed. Blackwell Science; Oxford, England: 2001.
-
- Darbari DS, Kple-Faget P, Kwagyan J, Rana S, Gordeuk VR, Castro O. Circumstances of death in adult sickle cell disease patients. Am J Hematol. 2006;81:858–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical