

Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery)
- PMID: 21228246
- PMCID: PMC3024330
- DOI: 10.2337/dc10-1407
Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery)
Abstract
Objective: The optimal treatment of hyperglycemia in general surgical patients with type 2 diabetes mellitus is not known.
Research design and methods: This randomized multicenter trial compared the safety and efficacy of a basal-bolus insulin regimen with glargine once daily and glulisine before meals (n = 104) to sliding scale regular insulin (SSI) four times daily (n = 107) in patients with type 2 diabetes mellitus undergoing general surgery. Outcomes included differences in daily blood glucose (BG) and a composite of postoperative complications including wound infection, pneumonia, bacteremia, and respiratory and acute renal failure.
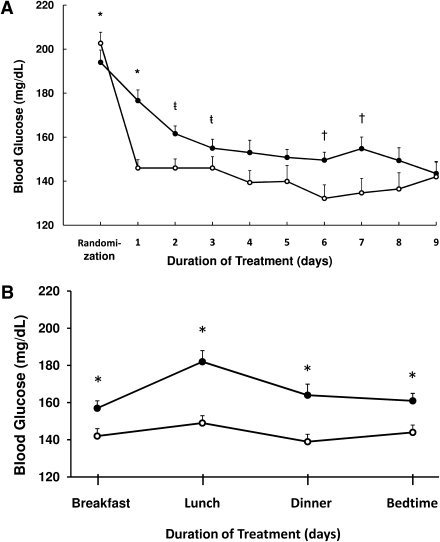
Results: The mean daily glucose concentration after the 1st day of basal-bolus insulin and SSI was 145 ± 32 mg/dL and 172 ± 47 mg/dL, respectively (P < 0.01). Glucose readings <140 mg/dL were recorded in 55% of patients in basal-bolus and 31% in the SSI group (P < 0.001). There were reductions with basal-bolus as compared with SSI in the composite outcome [24.3 and 8.6%; odds ratio 3.39 (95% CI 1.50-7.65); P = 0.003]. Glucose <70 mg/dL was reported in 23.1% of patients in the basal-bolus group and 4.7% in the SSI group (P < 0.001), but there were no significant differences in the frequency of BG <40 mg/dL between groups (P = 0.057).
Conclusions: Basal-bolus treatment with glargine once daily plus glulisine before meals improved glycemic control and reduced hospital complications compared with SSI in general surgery patients. Our study indicates that a basal-bolus insulin regimen is preferred over SSI in the hospital management of general surgery patients with type 2 diabetes.
Trial registration: ClinicalTrials.gov NCT00596687.
Figures
References
-
- Clement S, Braithwaite SS, Magee MF, et al. American Diabetes Association Diabetes in Hospitals Writing Committee Management of diabetes and hyperglycemia in hospitals. Diabetes Care 2004;27:553–591 - PubMed
-
- Smiley DD, Umpierrez GE. Perioperative glucose control in the diabetic or nondiabetic patient. South Med J 2006;99:580–591 - PubMed
-
- Lazar HL, Chipkin SR, Fitzgerald CA, Bao Y, Cabral H, Apstein CS. Tight glycemic control in diabetic coronary artery bypass graft patients improves perioperative outcomes and decreases recurrent ischemic events. Circulation 2004;109:1497–1502 - PubMed
-
- Ramos M, Khalpey Z, Lipsitz S, et al. Relationship of perioperative hyperglycemia and postoperative infections in patients who undergo general and vascular surgery. Ann Surg 2008;248:585–591 - PubMed
-
- Risum O, Abdelnoor M, Svennevig JL, et al. Diabetes mellitus and morbidity and mortality risks after coronary artery bypass surgery. Scand J Thorac Cardiovasc Surg 1996;30:71–75 - PubMed
