

Non-HDL cholesterol shows improved accuracy for cardiovascular risk score classification compared to direct or calculated LDL cholesterol in a dyslipidemic population
- PMID: 21228254
- PMCID: PMC4684263
- DOI: 10.1373/clinchem.2010.154773
Non-HDL cholesterol shows improved accuracy for cardiovascular risk score classification compared to direct or calculated LDL cholesterol in a dyslipidemic population
Abstract
Background: Our objective was to evaluate the accuracy of cardiovascular disease (CVD) risk score classification by direct LDL cholesterol (dLDL-C), calculated LDL cholesterol (cLDL-C), and non-HDL cholesterol (non-HDL-C) compared to classification by reference measurement procedures (RMPs) performed at the CDC.
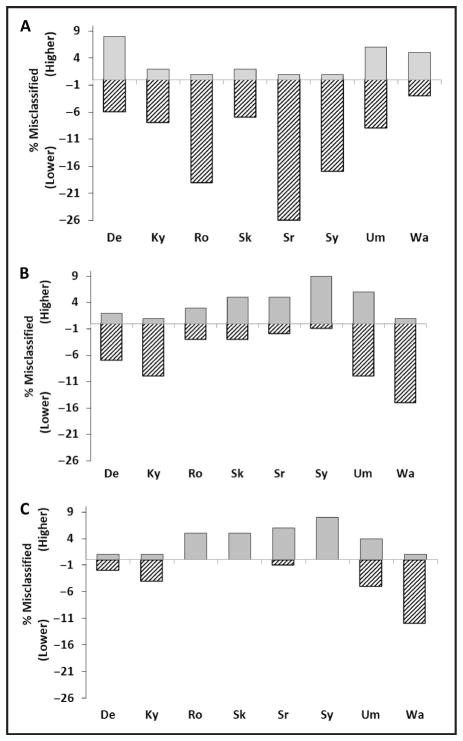
Methods: We examined 175 individuals, including 138 with CVD or conditions that may affect LDL-C measurement. dLDL-C measurements were performed using Denka, Kyowa, Sekisui, Serotec, Sysmex, UMA, and Wako reagents. cLDL-C was calculated by the Friedewald equation, using each manufacturer's direct HDL-C assay measurements, and total cholesterol and triglyceride measurements by Roche and Siemens (Advia) assays, respectively.
Results: For participants with triglycerides<2.26 mmol/L (<200 mg/dL), the overall misclassification rate for the CVD risk score ranged from 5% to 17% for cLDL-C methods and 8% to 26% for dLDL-C methods when compared to the RMP. Only Wako dLDL-C had fewer misclassifications than its corresponding cLDL-C method (8% vs 17%; P<0.05). Non-HDL-C assays misclassified fewer patients than dLDL-C for 4 of 8 methods (P<0.05). For participants with triglycerides≥2.26 mmol/L (≥200 mg/dL) and<4.52 mmol/L (<400 mg/dL), dLDL-C methods, in general, performed better than cLDL-C methods, and non-HDL-C methods showed better correspondence to the RMP for CVD risk score than either dLDL-C or cLDL-C methods.
Conclusions: Except for hypertriglyceridemic individuals, 7 of 8 dLDL-C methods failed to show improved CVD risk score classification over the corresponding cLDL-C methods. Non-HDL-C showed overall the best concordance with the RMP for CVD risk score classification of both normal and hypertriglyceridemic individuals.
Conflict of interest statement
Employment or Leadership: W.G. Miller,Clinical Chemistry , AACC; G.L. Myers, AACC.Consultant or Advisory Role: None declared.Stock Ownership: None declared.Honoraria: None declared.Research Funding: G. Miller, principal investigator for the project: Denka Seiken, Kyowa Medex, Sekisui Medical, Serotec, Sysmex International Reagents, UMA, and Wako Pure Chemical Industries donated reagents, calibrators, and controls and contributed financial support to Pacific Biometrics Research Foundation. Genzyme and Pointe Scientific contributed financial support to Pacific Biometrics Research Foundation. Pacific Biometrics Research Foundation provided a grant to Virginia Commonwealth University (funded by the financial contributions noted above). Roche Diagnostics donated reagents, calibrators, controls, and a Hitachi 917 instrument. H.E. van Deventer, Warren Grant Magnuson Clinical Center, Intramural Research Program of the National Institutes of Health. A.T. Remaley, Warren Grant Magnuson Clinical Center, Intramural Research Program of the National Institutes of Health.
Figures
References
-
- Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285:2486–97. - PubMed
-
- Nauck M, Warnick GR, Rifai N. Methods for measurement of LDL-cholesterol: a critical assessment of direct measurement by homogeneous assays versus calculation. Clin Chem. 2002;48:236–54. - PubMed
-
- Nauck M, Wiebe D, Warnick GR. Measurement of high-density-lipoprotein cholesterol. In: Rifai N, Warnick GR, Dominiczak MH, editors. Handbook of lipoprotein testing. 2. Washington, DC: AACC Press; 2000. pp. 227–30.
-
- Gordon T, Kannel WB, Castelli WP, Dawber TR. Lipoproteins, cardiovascular disease, and death. The Framingham study. Arch Intern Med. 1981;141:1128–31. - PubMed
-
- Castelli WP, Doyle JT, Gordon T, Hames CG, Hjortland MC, Hulley SB, et al. HDL cholesterol and other lipids in coronary heart disease. The cooperative lipoprotein phenotyping study. Circulation. 1977;55:767–72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
