

Genetic and epigenetic alterations during renal carcinogenesis
- PMID: 21228928
- PMCID: PMC3016104
Genetic and epigenetic alterations during renal carcinogenesis
Abstract
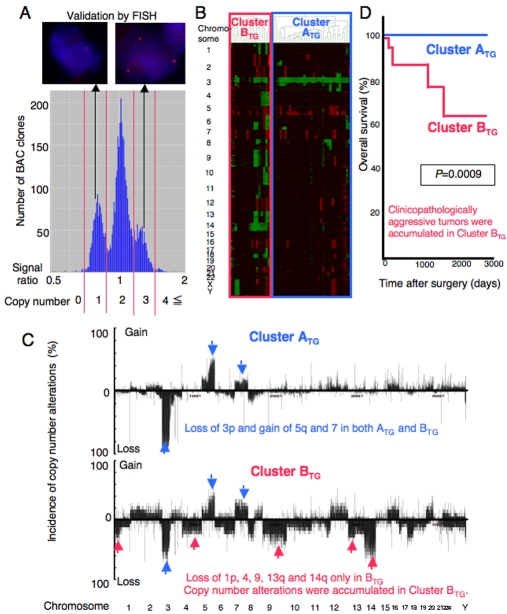
Renal cell carcinoma (RCC) is not a single entity, but comprises a group of tumors including clear cell RCC, papillary RCC and chromophobe RCC, which arise from the epithelium of renal tubules. The majority of clear cell RCCs, the major histological subtype, have genetic or epigenetic inactivation of the von Hippel-Lindau (VHL) gene. Germline mutations in the MET and fumarate hydratase (FH) genes lead to the development of type 1 and type 2 papillary RCCs, respectively, and such mutations of either the TSC1 or TSC2 gene increase the risk of RCC. Genome-wide copy number alteration analysis has suggested that loss of chromosome 3p and gain of chromosomes 5q and 7 may be copy number aberrations indispensable for the development of clear cell RCC. When chromosome 1p, 4, 9, 13q or 14q is also lost, more clinicopathologically aggressive clear cell RCC may develop. Since renal carcinogenesis is associated with neither chronic inflammation nor persistent viral infection, and hardly any histological change is evident in corresponding non-tumorous renal tissue from patients with renal tumors, precancerous conditions in the kidney have been rarely described. However, regional DNA hypermethylation on C-type CpG islands has already accumulated in such non-cancerous renal tissues, suggesting that, from the viewpoint of altered DNA methylation, the presence of precancerous conditions can be recognized even in the kidney. Genome-wide DNA methylation profiles in precancerous conditions are basically inherited by the corresponding clear cell RCCs developing in individual patients: DNA methylation alterations at the precancerous stage may further predispose renal tissue to epigenetic and genetic alterations, generate more malignant cancers, and even determine patient outcome. The list of tumor-related genes silenced by DNA hypermethylation has recently been increasing. Genetic and epigenetic profiling provides an optimal means of prognostication for patients with RCCs. Recently developed high-throughput technologies for genetic and epigenetic analyses will further accelerate the identification of key molecules for use in the prevention, diagnosis and therapy of RCCs.
Keywords: DNA methylation; Renal cell carcinoma; copy number alteration; precancerous condition; prognostication.
Figures


References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. in press; DOI: 10.1002/ijc.25516. - DOI - PubMed
-
- Baldewijns MM, van Vlodrop IJ, Schouten LJ, Soetekouw PM, de Bruine AP, van Engeland M. Genetics and epigenetics of renal cell cancer. Biochim Biophys Acta. 2008;1785:133–155. - PubMed
-
- Lopez-Beltran A, Carrasco JC, Cheng L, Scarpelli M, Kirkali Z, Montironi R. 2009 update on the classification of renal epithelial tumors in adults. Int J Urol. 2009;16:432–443. - PubMed
-
- Eble JN, Togashi K, Pisani P. Renal cell carcinoma. In “World Health Organization classification of tumours. Pathology and genetics. Tumours of the urinary system and male genital organs”. Lyon: IARC Press; 2004. pp. 10–43.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous