

Left-ventricular systolic and diastolic dyssynchrony as assessed by multi-harmonic phase analysis of gated SPECT myocardial perfusion imaging in patients with end-stage renal disease and normal LVEF
- PMID: 21229401
- PMCID: PMC3077281
- DOI: 10.1007/s12350-010-9331-2
Left-ventricular systolic and diastolic dyssynchrony as assessed by multi-harmonic phase analysis of gated SPECT myocardial perfusion imaging in patients with end-stage renal disease and normal LVEF
Abstract
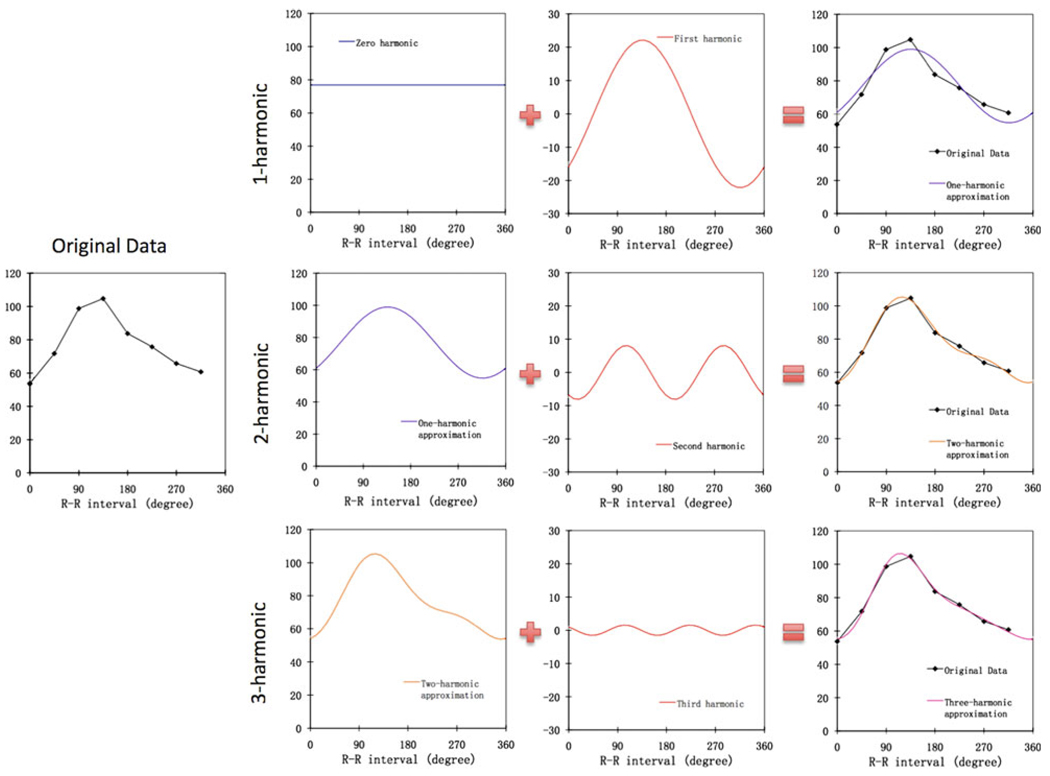
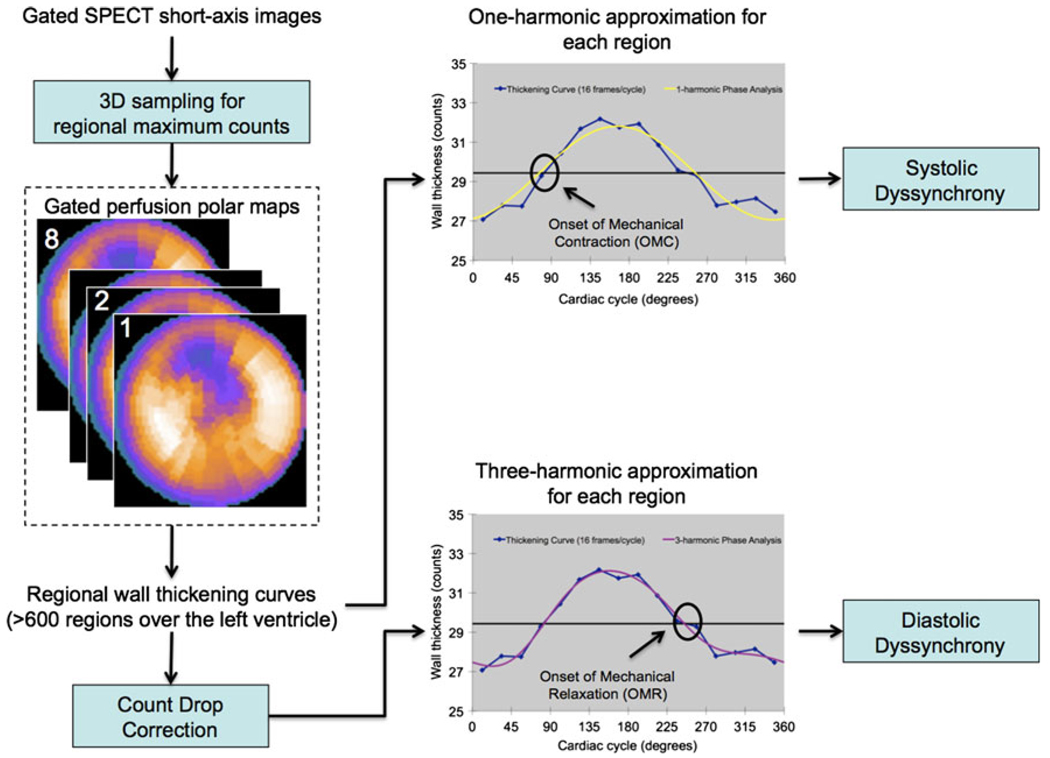
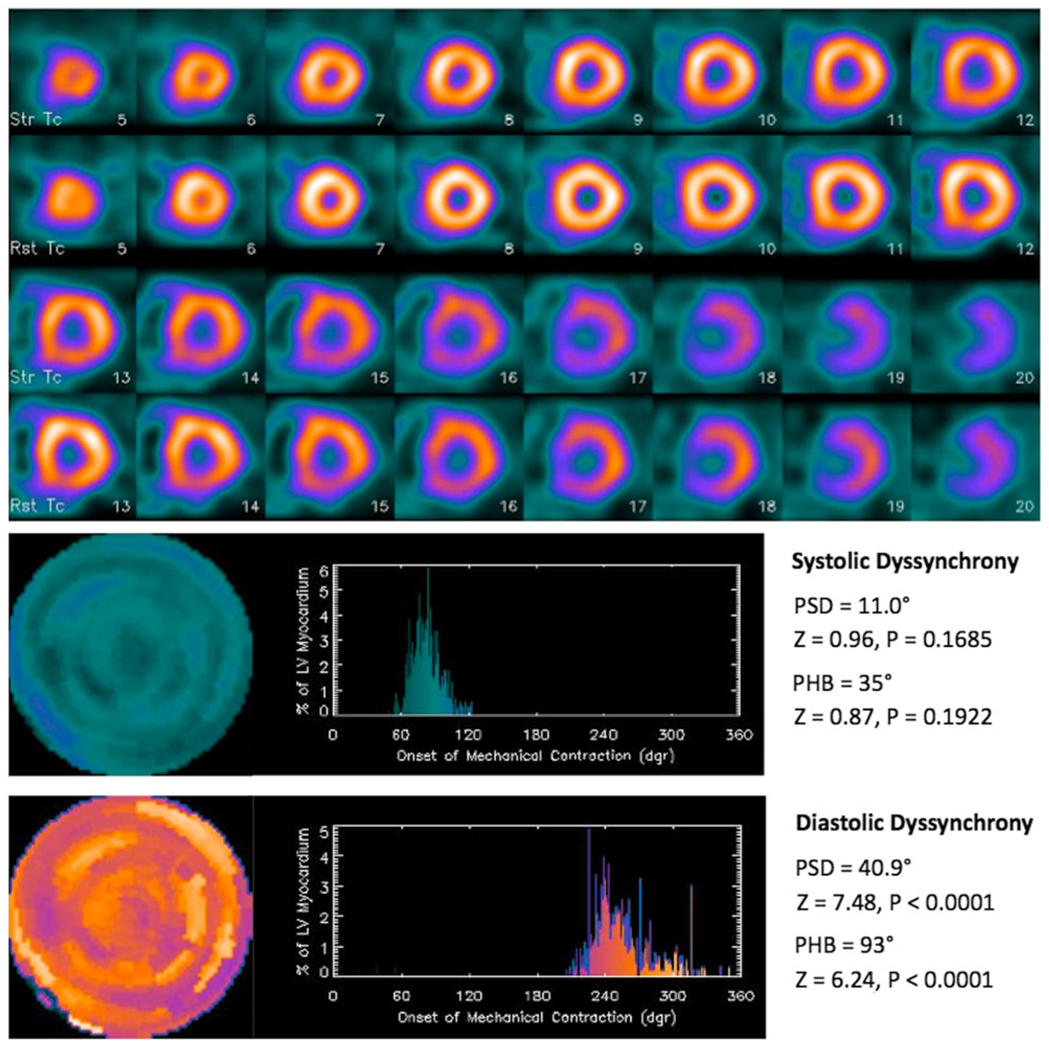
Background: The purpose of this study was to develop a multi-harmonic phase analysis method to measure diastolic dyssynchrony from conventional gated SPECT myocardial perfusion imaging (MPI) data and to compare it with systolic dyssynchrony in normal subjects and in patients with end-stage renal disease (ESRD) and normal left-ventricular ejection fraction (LVEF).
Methods: 121 consecutive patients with ESRD and normal LVEF and 30 consecutive normal controls were enrolled. Diastolic dyssynchrony parameters were calculated using 3-harmonic phase analysis. Systolic dyssynchrony parameters were calculated using the established 1-harmonic phase analysis.
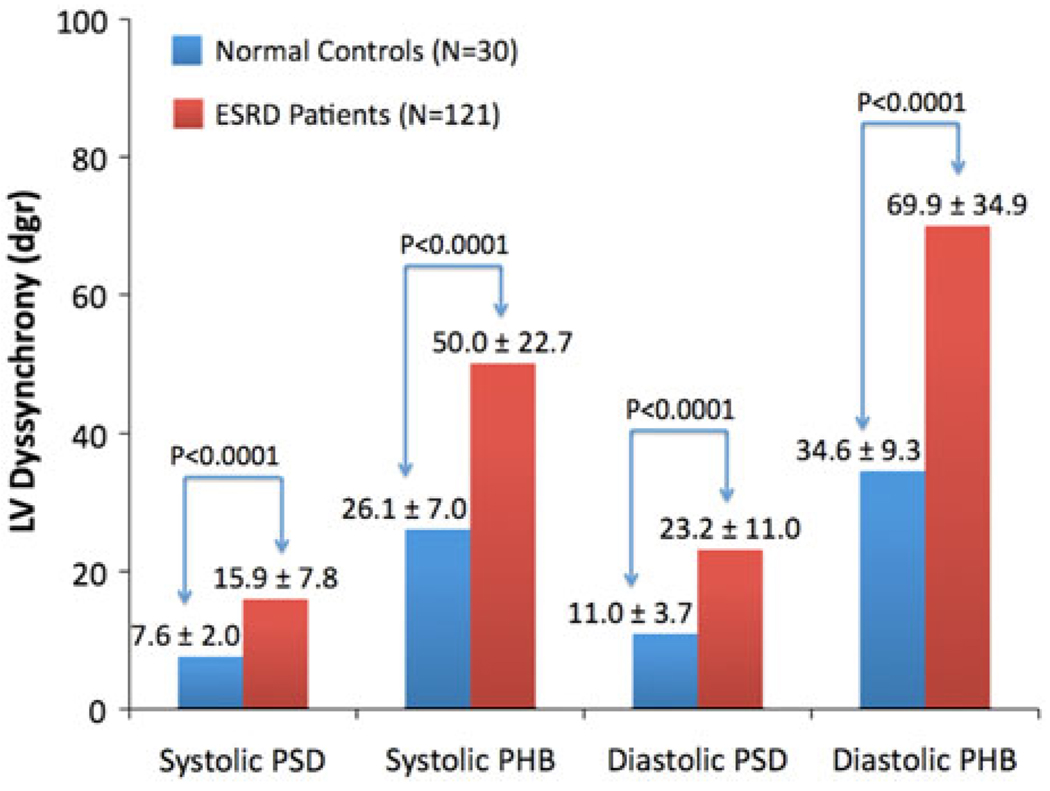
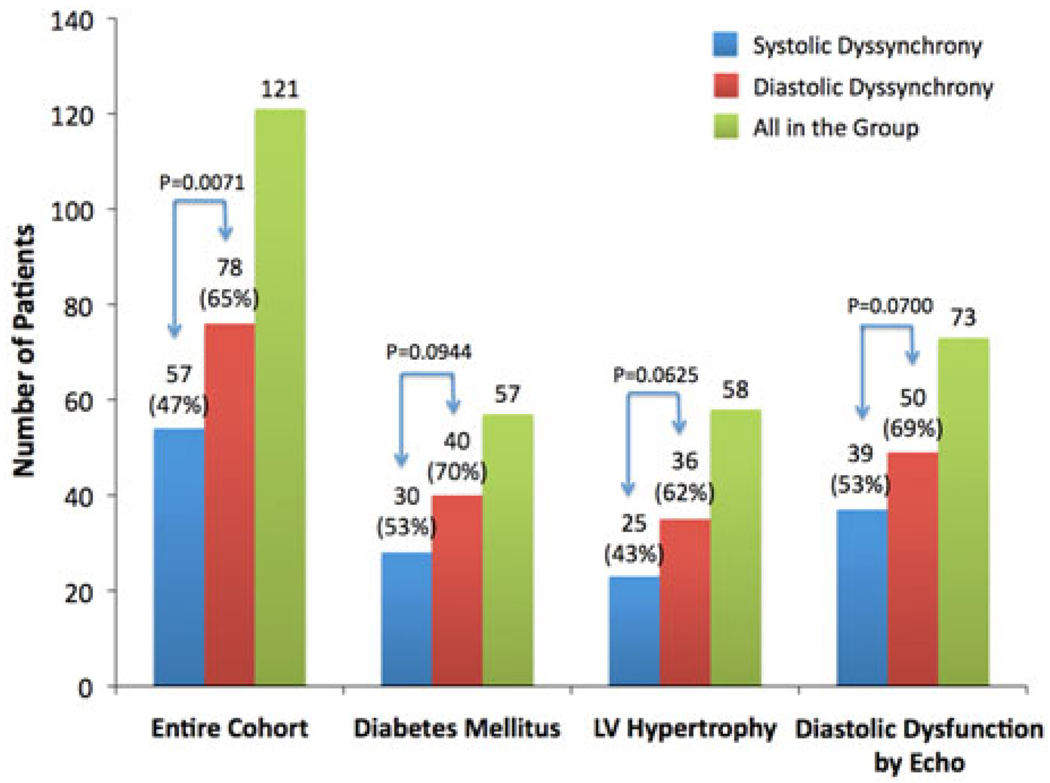
Results: The systolic and diastolic dyssynchrony parameters were correlated, but significantly different in both control and ESRD groups, indicating they were physiologically related but measured different LV mechanisms. The systolic and diastolic dyssynchrony parameters were each significantly different between the control and the ESRD groups. Significant systolic and diastolic dyssynchrony were found in 47% and 65% of the entire ESRD group.
Conclusion: Multi-harmonic phase analysis has been developed to assess diastolic dyssynchrony, which measured a new LV mechanism of regional function from gated SPECT MPI and showed a significantly higher prevalence rate than systolic dyssynchrony in patients with ESRD and normal LVEF.
Conflict of interest statement
The terms of this arrangement have been reviewed and approved by Emory University in accordance with its conflict-of-interest practice.
Figures
References
-
- Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108:2154–2169. - PubMed
-
- Verma A, Anavekar NS, Meris A, et al. The relationship between renal function and cardiac structure, function and prognosis after myocardial infarction. The VALIANT Echo Study. J Am Coll Cardiol. 2007;50:1238–1245. - PubMed
-
- Foley RN, Parfrey PS, Harnett JD, et al. Clinical and echocardiographic disease in patients starting end-stage renal disease therapy. Kidney Int. 1995;47:186–192. - PubMed
-
- Curtis BM, Parfrey PS. Congestive heart failure in chronic kidney disease: Disease-specific mechanisms of systolic and diastolic heart failure and management. Cardiol Clin. 2005;23:275–284. - PubMed
-
- Hayashi SY, Seeberger A, Lind B, Nowak J, do Nascimento MM, Lindholm B, et al. A single session of haemodialysis improves left ventricular synchronicity in patients with end-stage renal disease: A pilot tissue synchronization imaging study. Nephrol Dial Transplant. 2008;23:3622–3628. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
