

Effect of conditioning regimen intensity on acute myeloid leukemia outcomes after umbilical cord blood transplantation
- PMID: 21232621
- PMCID: PMC4130206
- DOI: 10.1016/j.bbmt.2011.01.007
Effect of conditioning regimen intensity on acute myeloid leukemia outcomes after umbilical cord blood transplantation
Abstract
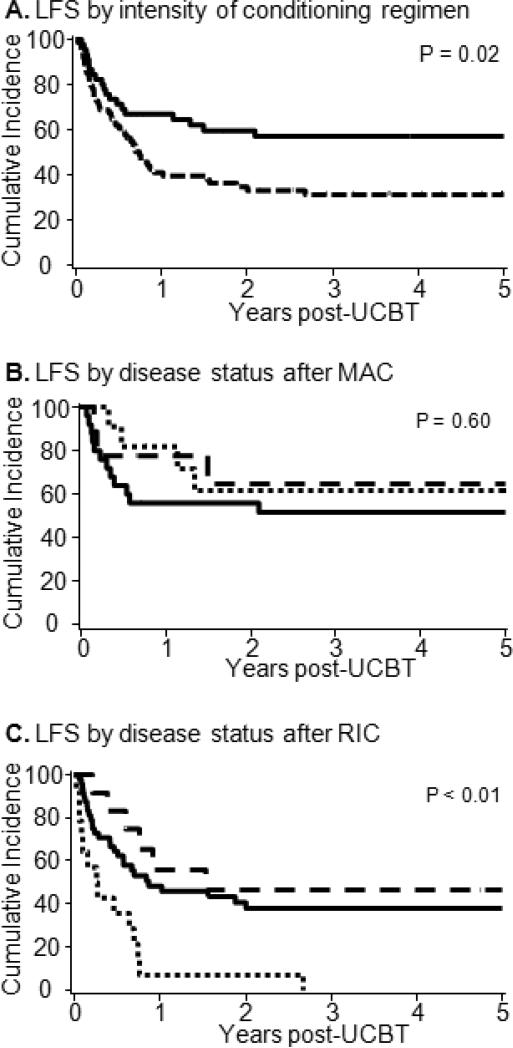
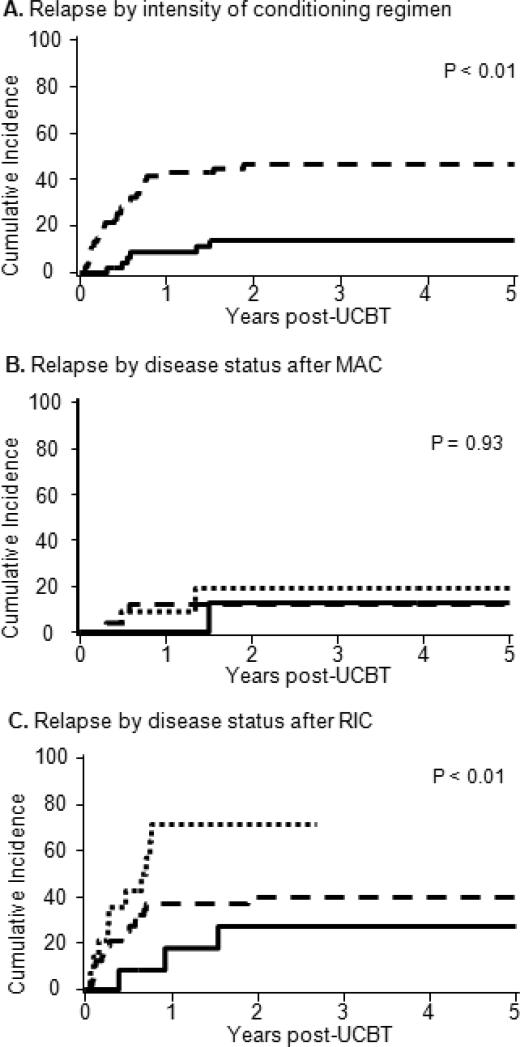
Reduced-intensity conditioning (RIC) umbilical cord blood (UCB) transplantation is increasingly used in hematopoietic stem cell transplantation (HCT) for older and medically unfit patients. Data on the efficacy of HCT after RIC relative to myeloablative conditioning (MAC) are limited. We compared the outcomes of acute myeloid leukemia (AML) patients >18 yrs who received UCB grafts after either RIC or MAC. One hundred nineteen adult patients with AML in complete remission (CR) underwent an UCB transplant after RIC (n =74, 62%) or MAC (n = 45, 38%) between January 2001 and December 2009. Conditioning was either reduced intensity and consisted of cyclophosphamide 50 mg/kg, fludarabine 200 mg/m(2), and total-body irradiation (TBI) 200 cGy or myelablative and consisted for cyclophosphamide 120 mg/kg, fludarabine 75 mg/m(2), and TBI 1200-1320 cGy. All patients received cyclosporine (day -3 to day +180) and mycophenolate mofetil (day -3 to day +45) post-HCT immunosuppression and hematopoietic growth factor. Use of RIC was reserved for patients >45 years (n = 66, 89%) or preexisting severe comorbidities (n = 8, 11%). The 2 groups were similar except for preceding myelodysplastic syndrome (RIC = 28% versus MAC = 4%, P < .01) and age that was dictated by the treatment protocols (median, RIC = 55 years versus MAC = 33years; P < .01). The incidence of neutrophil recovery at day +42 was higher with RIC (94% versus MAC = 82%, P < .1), whereas platelet recovery at the sixth month was similar (RIC = 68% versus MAC = 67%, P = .30). Incidence of grade II-IV acute graft-versus-host disease (aGVHD) (RIC = 47% versus MAC = 67%, P < .01) was decreased with similar incidence of chronic GVHD (cGVHD) (RIC = 30% versus MAC = 34%, P = .43). Median follow-up for survivors was 3.8 and 4.5 years for RIC and MAC, respectively (P = .4). Using RIC, 3-year leukemia-free survival (LFS) was decreased (31% versus MAC = 55%, P = .02) and 3-year relapse incidence was increased (43% versus MAC = 9%, P < .01). Two-year transplant-related mortality (TRM) was similar (RIC = 19% versus MAC = 27%; P = .55). In multivariate analysis, RIC recipients and those in CR2 with CR1 duration <1 year had higher risk of relapse and poorer LFS with no independent predictors of TRM. UCB with RIC extends the use of allogeneic HCT for older and frail patients without excessive TRM with greater benefit for patients in CR1 and CR2 with longer CR1.
Copyright © 2011 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Thiotepa-Based Intensified Reduced-Intensity Conditioning Adult Double-Unit Cord Blood Hematopoietic Stem Cell Transplantation Results in Decreased Relapse Rate and Improved Survival Compared with Transplantation Following Standard Reduced-Intensity Conditioning: A Retrospective Cohort Comparison.Biol Blood Marrow Transplant. 2018 Aug;24(8):1671-1677. doi: 10.1016/j.bbmt.2018.04.019. Epub 2018 Apr 21. Biol Blood Marrow Transplant. 2018. PMID: 29684565
-
Reduced-intensity allogeneic transplant in patients older than 55 years: unrelated umbilical cord blood is safe and effective for patients without a matched related donor.Biol Blood Marrow Transplant. 2008 Mar;14(3):282-9. doi: 10.1016/j.bbmt.2007.12.488. Biol Blood Marrow Transplant. 2008. PMID: 18275894 Free PMC article. Clinical Trial.
-
Myeloablative Versus Reduced-Intensity Hematopoietic Cell Transplantation for Acute Myeloid Leukemia and Myelodysplastic Syndromes.J Clin Oncol. 2017 Apr 10;35(11):1154-1161. doi: 10.1200/JCO.2016.70.7091. Epub 2017 Feb 13. J Clin Oncol. 2017. PMID: 28380315 Free PMC article. Clinical Trial.
-
Comparison of reduced-intensity and myeloablative conditioning regimens for allogeneic hematopoietic stem cell transplantation in patients with acute myeloid leukemia and acute lymphoblastic leukemia: a meta-analysis.Stem Cells Dev. 2014 Nov 1;23(21):2535-52. doi: 10.1089/scd.2014.0123. Epub 2014 Sep 17. Stem Cells Dev. 2014. PMID: 25072307 Free PMC article. Review.
-
Pushing the envelope-nonmyeloablative and reduced intensity preparative regimens for allogeneic hematopoietic transplantation.Bone Marrow Transplant. 2015 Sep;50(9):1157-67. doi: 10.1038/bmt.2015.61. Epub 2015 May 18. Bone Marrow Transplant. 2015. PMID: 25985053 Free PMC article. Review.
Cited by
-
A novel reduced-intensity conditioning regimen induces a high incidence of sustained donor-derived neutrophil and platelet engraftment after double-unit cord blood transplantation.Biol Blood Marrow Transplant. 2013 May;19(5):799-803. doi: 10.1016/j.bbmt.2013.02.007. Epub 2013 Feb 14. Biol Blood Marrow Transplant. 2013. PMID: 23416850 Free PMC article.
-
A comparison of immune reconstitution and graft-versus-host disease following myeloablative conditioning versus reduced toxicity conditioning and umbilical cord blood transplantation in paediatric recipients.Br J Haematol. 2011 Oct;155(2):218-34. doi: 10.1111/j.1365-2141.2011.08822.x. Epub 2011 Aug 16. Br J Haematol. 2011. PMID: 21848882 Free PMC article.
-
Ex Vivo Mesenchymal Precursor Cell-Expanded Cord Blood Transplantation after Reduced-Intensity Conditioning Regimens Improves Time to Neutrophil Recovery.Biol Blood Marrow Transplant. 2017 Aug;23(8):1359-1366. doi: 10.1016/j.bbmt.2017.05.002. Epub 2017 May 12. Biol Blood Marrow Transplant. 2017. PMID: 28506845 Free PMC article. Clinical Trial.
-
The development of a myeloablative, reduced-toxicity, conditioning regimen for cord blood transplantation.Clin Lymphoma Myeloma Leuk. 2014 Feb;14(1):e1-5. doi: 10.1016/j.clml.2013.08.006. Epub 2013 Oct 26. Clin Lymphoma Myeloma Leuk. 2014. PMID: 24169268 Free PMC article.
-
A phase I/II trial of intrabone marrow cord blood transplantation and comparison of the hematological recovery with the Japanese nationwide database.Bone Marrow Transplant. 2017 Apr;52(4):574-579. doi: 10.1038/bmt.2016.319. Epub 2017 Jan 9. Bone Marrow Transplant. 2017. PMID: 28067880 Clinical Trial.
References
-
- Cornelissen JJ, van Putten WL, Verdonck LF, et al. Results of a HOVON/SAKK donor versus no-donor analysis of myeloablative HLA-identical sibling stem cell transplantation in first remission acute myeloid leukemia in young and middle-aged adults: benefits for whom? Blood. 2007;109:3658–66. - PubMed
-
- Forman SJ. What is the role of reduced-intensity transplantation in the treatment of older patients with AML? Hematology Am Soc Hematol Educ Program. 2009:406–13. - PubMed
-
- Baron F, Storb R, Storer BE, et al. Factors associated with outcomes in allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning after failed myeloablative hematopoietic cell transplantation. J Clin Oncol. 2006;24:4150–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
