

Suppression of re-entrant and multifocal ventricular fibrillation by the late sodium current blocker ranolazine
- PMID: 21232675
- PMCID: PMC4344130
- DOI: 10.1016/j.jacc.2010.07.045
Suppression of re-entrant and multifocal ventricular fibrillation by the late sodium current blocker ranolazine
Abstract
Objectives: The purpose of this study was to test the hypothesis that the late Na current blocker ranolazine suppresses re-entrant and multifocal ventricular fibrillation (VF).
Background: VF can be caused by either re-entrant or focal mechanism.
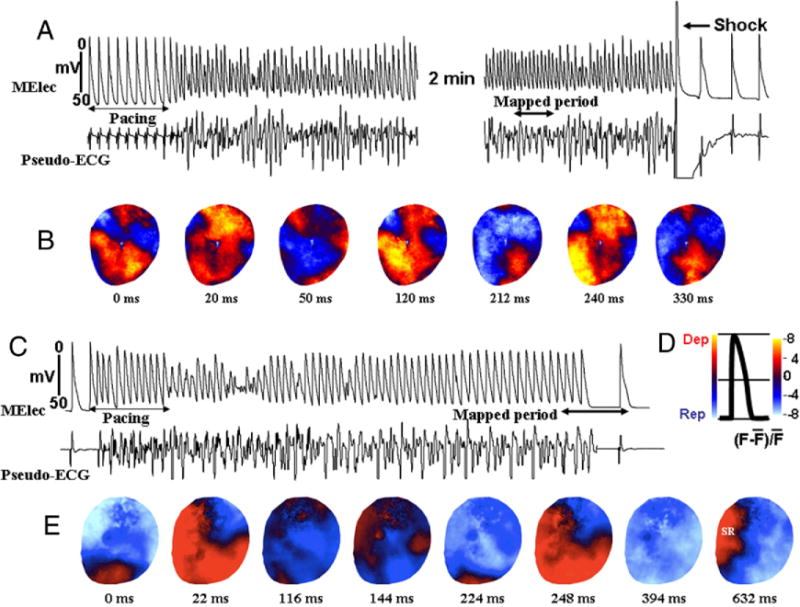
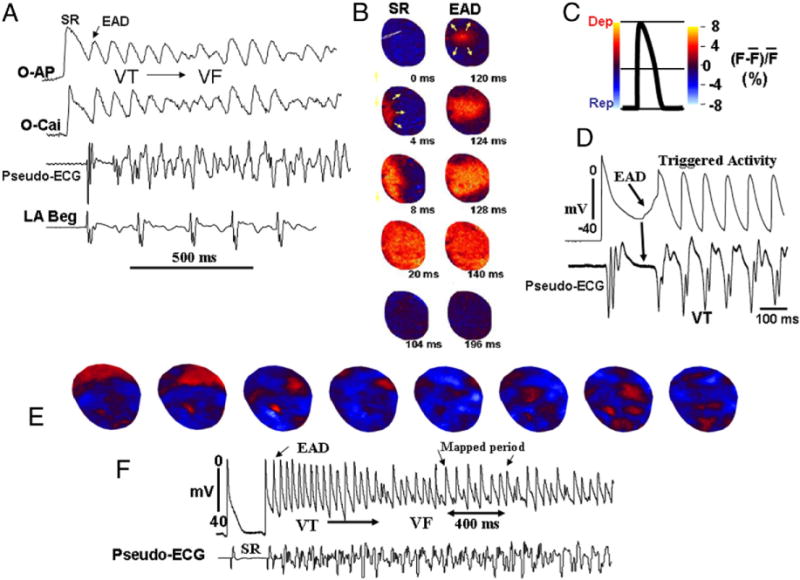
Methods: Simultaneous voltage and intracellular Ca(+)² optical mapping of the left ventricular epicardial surface along with microelectrode recordings was performed in 24 isolated-perfused aged rat hearts. Re-entrant VF was induced by rapid pacing and multifocal VF by exposure to oxidative stress with 0.1 mM hydrogen peroxide (H₂O₂).
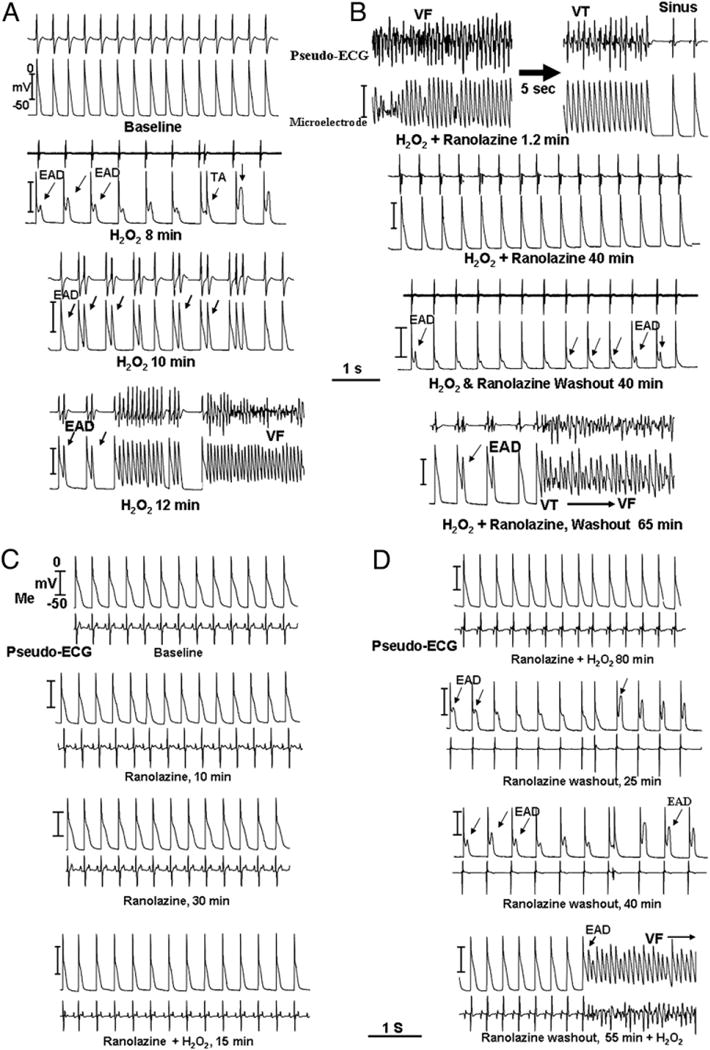
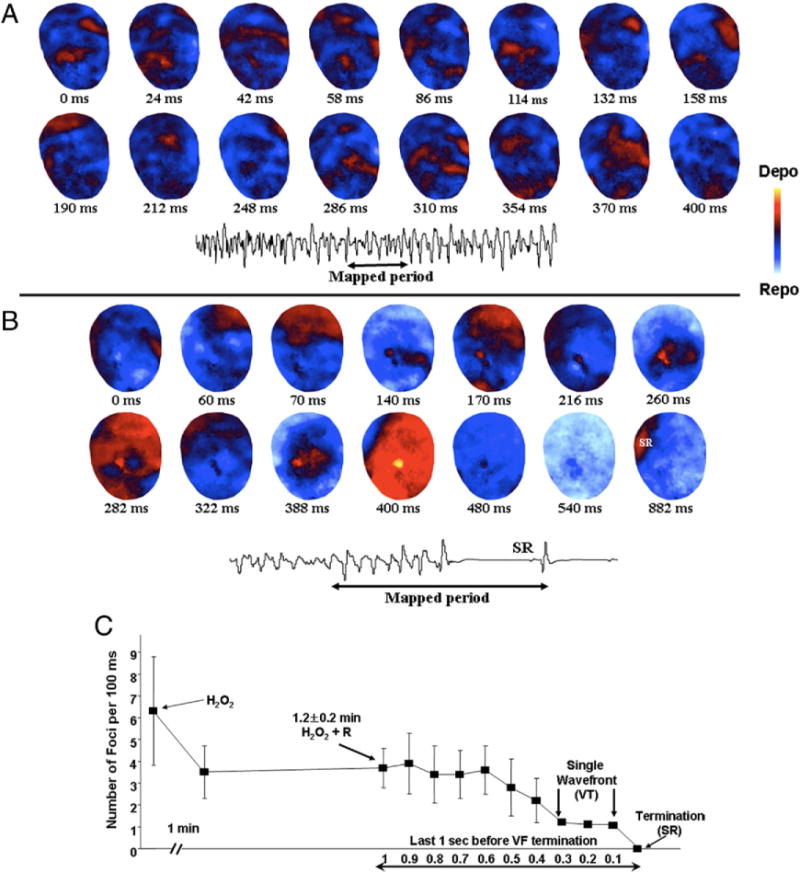
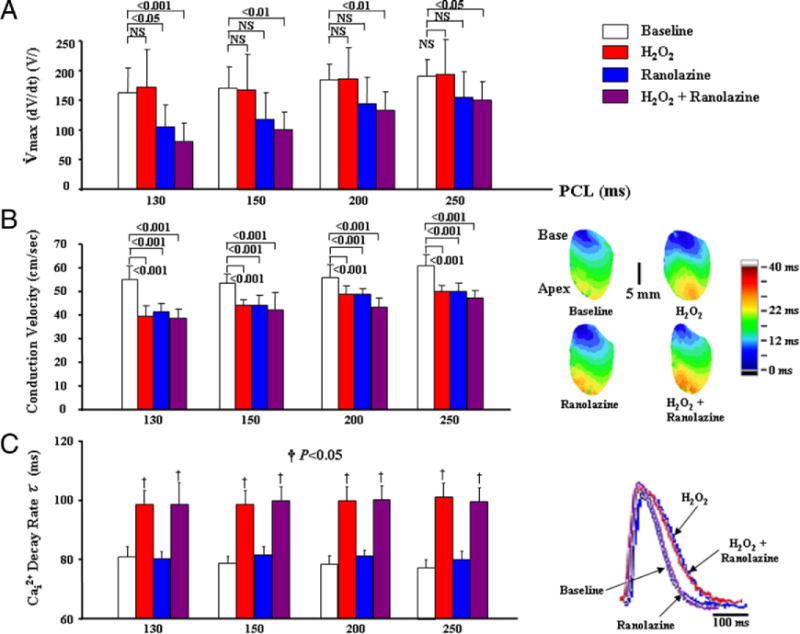
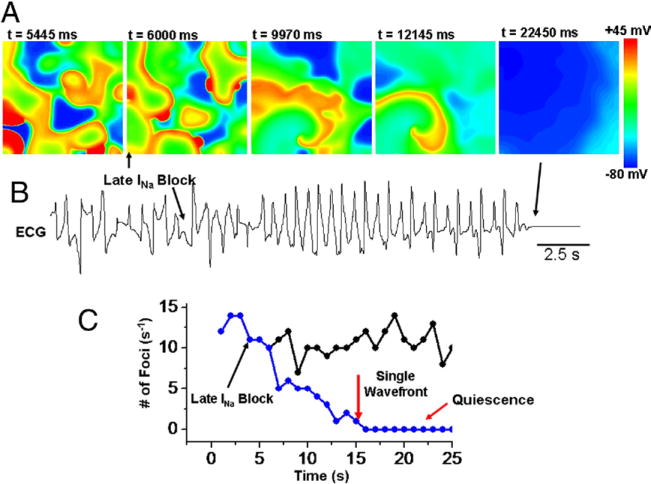
Results: Rapid pacing induced sustained VF in 7 of 8 aged rat hearts, characterized by 2 to 4 broad propagating wavefronts. Ranolazine significantly (p < 0.05) reduced the maximum slope of action potential duration restitution curve and converted sustained to nonsustained VF lasting 24 ± 8 s in all 7 hearts. Exposure to H₂O₂ initiated early afterdepolarization (EAD)-mediated triggered activity that led to sustained VF in 8 out of 8 aged hearts. VF was characterized by multiple foci, appearing at an average of 6.8 ± 3.2 every 100 ms, which remained confined to a small area averaging 2.8 ± 0.85 mm² and became extinct after a mean of 43 ± 16 ms. Ranolazine prevented (when given before H₂O₂) and suppressed H₂O₂-mediated EADs by reducing the number of foci, causing VF to terminate in 8 out of 8 hearts. Simulations in 2-dimensional tissue with EAD-mediated multifocal VF showed progressive reduction in the number of foci and VF termination by blocking the late Na current.
Conclusions: Late Na current blockade with ranolazine is effective at suppressing both pacing-induced re-entrant VF and EAD-mediated multifocal VF.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Selective inhibition of late sodium current suppresses ventricular tachycardia and fibrillation in intact rat hearts.Heart Rhythm. 2014 Mar;11(3):492-501. doi: 10.1016/j.hrthm.2013.11.026. Epub 2013 Nov 28. Heart Rhythm. 2014. PMID: 24291413 Free PMC article.
-
Glycolytic inhibition causes spontaneous ventricular fibrillation in aged hearts.Am J Physiol Heart Circ Physiol. 2011 Jul;301(1):H180-91. doi: 10.1152/ajpheart.00128.2011. Epub 2011 Apr 8. Am J Physiol Heart Circ Physiol. 2011. PMID: 21478408 Free PMC article.
-
Antifibrillatory effect of ranolazine during severe coronary stenosis in the intact porcine model.Heart Rhythm. 2011 Apr;8(4):608-14. doi: 10.1016/j.hrthm.2010.11.029. Epub 2010 Nov 19. Heart Rhythm. 2011. PMID: 21094698
-
Mechanisms of ranolazine's dual protection against atrial and ventricular fibrillation.Europace. 2013 Mar;15(3):317-24. doi: 10.1093/europace/eus380. Epub 2012 Dec 7. Europace. 2013. PMID: 23220484 Free PMC article. Review.
-
Ranolazine: clinical applications and therapeutic basis.Am J Cardiovasc Drugs. 2013 Feb;13(1):5-16. doi: 10.1007/s40256-012-0003-2. Am J Cardiovasc Drugs. 2013. PMID: 23335347 Review.
Cited by
-
Bifurcation theory and cardiac arrhythmias.Am J Cardiovasc Dis. 2013;3(1):1-16. Epub 2013 Feb 17. Am J Cardiovasc Dis. 2013. PMID: 23459417 Free PMC article.
-
Mitochondrial Dysfunction-Associated Arrhythmogenic Substrates in Diabetes Mellitus.Front Physiol. 2018 Dec 6;9:1670. doi: 10.3389/fphys.2018.01670. eCollection 2018. Front Physiol. 2018. PMID: 30574091 Free PMC article. Review.
-
18β-Glycyrrhetinic acid preferentially blocks late Na current generated by ΔKPQ Nav1.5 channels.Acta Pharmacol Sin. 2012 Jun;33(6):752-60. doi: 10.1038/aps.2012.22. Epub 2012 May 21. Acta Pharmacol Sin. 2012. PMID: 22609834 Free PMC article.
-
Antiarrhythmic Drug Therapy to Avoid Implantable Cardioverter Defibrillator Shocks.Arrhythm Electrophysiol Rev. 2016 Aug;5(2):117-21. doi: 10.15420/AER.2016.10.2. Arrhythm Electrophysiol Rev. 2016. PMID: 27617090 Free PMC article.
-
The electrical restitution of the non-propagated cardiac ventricular action potential.Pflugers Arch. 2024 Jan;476(1):9-37. doi: 10.1007/s00424-023-02866-0. Epub 2023 Oct 3. Pflugers Arch. 2024. PMID: 37783868 Free PMC article. Review.
References
-
- Moe GK, Rheinboldt WL, Abildskov JA. A computer model of atrial fibrillation. Am Heart J. 1964;64:200–20. - PubMed
-
- Samie FH, Berenfeld O, Anumonwo J, et al. Rectification of the background potassium current: a determinant of rotor dynamics in ventricular fibrillation. Circ Res. 2001;89:1216–23. - PubMed
-
- Wu TJ, Lin SF, Weiss JN, Ting CT, Chen PS. Two types of ventricular fibrillation in isolated rabbit hearts: importance of excitability and action potential duration restitution. Circulation. 2002;106:1859–66. - PubMed
-
- Scherf D. Studies on auricular tachycardia caused by aconitine administration. Proc Exp Biol Med. 1947;64:233–9. - PubMed
-
- Swissa M, Qu Z, Ohara T, et al. Action potential duration restitution and ventricular fibrillation due to rapid focal excitation. Am J Physiol Heart Circ Physiol. 2002;282:H1915–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
