

Collateral flow predicts response to endovascular therapy for acute ischemic stroke
- PMID: 21233472
- PMCID: PMC3051344
- DOI: 10.1161/STROKEAHA.110.595256
Collateral flow predicts response to endovascular therapy for acute ischemic stroke
Abstract
Background and purpose: Collaterals sustain the penumbra before recanalization and offset infarct growth, yet the influence of baseline collateral flow on recanalization after endovascular therapy remains relatively unexplored.
Methods: We analyzed consecutive patients who received endovascular therapy for acute cerebral ischemia from 2 distinct study populations. We assessed the relationship between pretreatment collateral grade and vascular recanalization (Thrombolysis In Myocardial Ischemia [TIMI] scale). In addition, we assessed infarct growth on serial MRI.
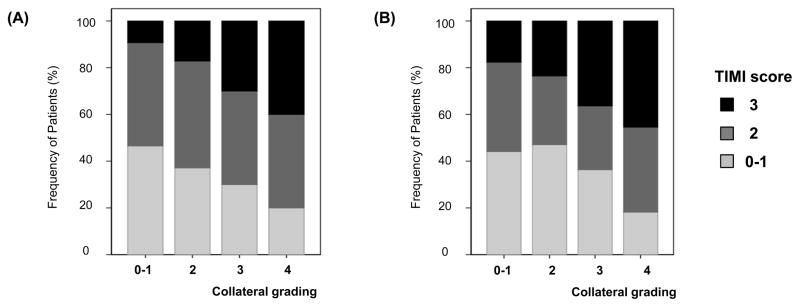
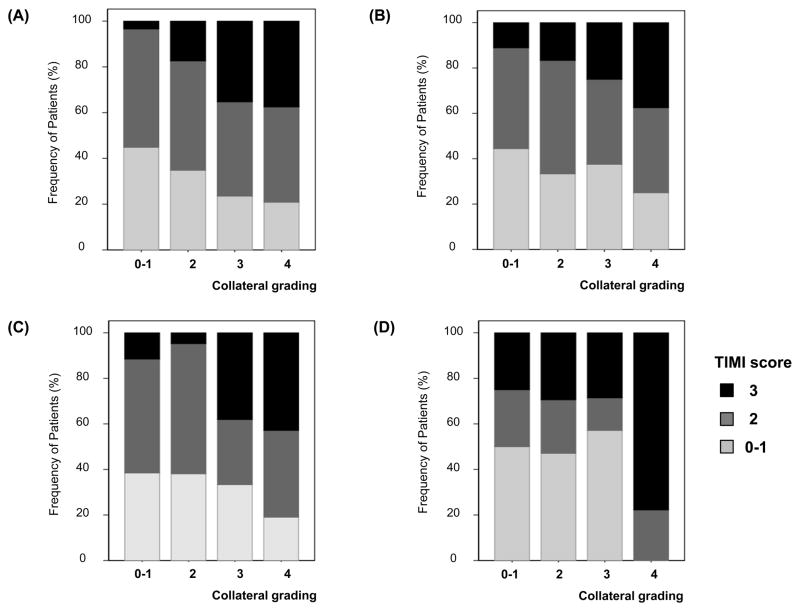
Results: A total of 222 patients was included, 138 from the United States and 84 from South Korea. Complete revascularization occurred in 14.1% (11 of 78) patients with poor pretreatment collateral grades, whereas it was observed in 25.2% (26 of 103) patients with good collaterals and 41.5% (17 of 41) patients with excellent collaterals (P<0.001). This relationship was consistently observed in both study populations, although the mode of endovascular therapy was different between them. After adjustment for other factors, including mode of endovascular therapy, prior use of intravenous tissue plasminogen activator, and site of occlusion, pretreatment collateral grade was independently associated with recanalization. When revascularization was achieved, greater infarct growth occurred in patients with poor collaterals than in those with good collaterals (P=0.012).
Conclusions: Our data indicate that angiographic collateral grade determines the recanalization rate after endovascular revascularization therapy. When therapeutic revascularization was achieved, beneficial effects were not observed in patients with poor collaterals. Angiographic collateral grade may therefore help guide treatment decision-making in acute cerebral ischemia.
Figures
References
-
- Powers WJ. Cerebral hemodynamics in ischemic cerebrovascular disease. Ann Neurol. 1991;29:231–240. - PubMed
-
- Liebeskind DS. Collateral circulation. Stroke. 2003;34:2279–2284. - PubMed
-
- Liebeskind DS. Collaterals in acute stroke: Beyond the clot. Neuroimaging Clin N Am. 2005;15:553–573. x. - PubMed
-
- Ringelstein EB, Biniek R, Weiller C, Ammeling B, Nolte PN, Thron A. Type and extent of hemispheric brain infarctions and clinical outcome in early and delayed middle cerebral artery recanalization. Neurology. 1992;42:289–298. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
