

The Effect of Race, Sex, and Insurance Status on Time-to-Listing Decisions for Liver Transplantation
- PMID: 21234099
- PMCID: PMC3014672
- DOI: 10.1155/2010/467976
The Effect of Race, Sex, and Insurance Status on Time-to-Listing Decisions for Liver Transplantation
Abstract
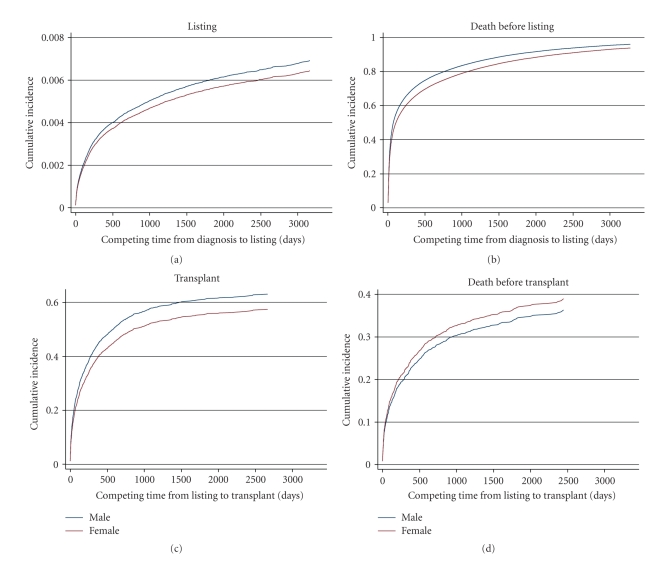
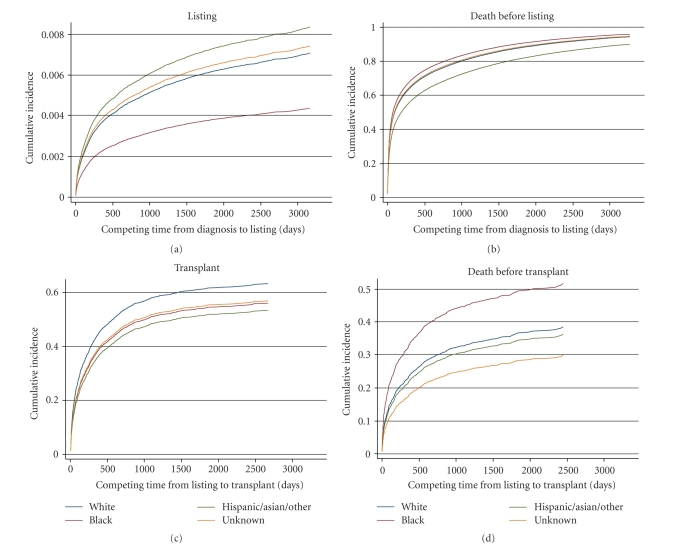
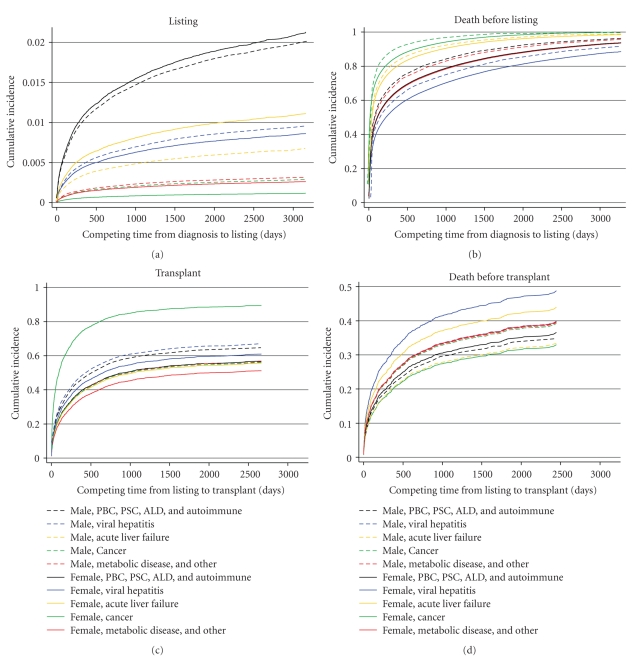
Fair allocation of organs to candidates listed for transplantation is fundamental to organ-donation policies. Processes leading to listing decisions are neither regulated nor understood. We explored whether patient characteristics affected timeliness of listing using population-based data on 144,507 adults hospitalized with liver-related disease in Pennsylvania. We linked hospitalizations to other secondary data and found 3,071 listed for transplants, 1,537 received transplants, and 57,020 died. Among candidates, 61% (n = 1,879) and 85.5% (n = 2,626) were listed within 1 and 3 years of diagnosis; 26.7% (n = 1,130) and 95% (n = 1,468) of recipients were transplanted within 1 and 3 years of listing. Using competing-risks models, we found few overall differences by sex, but both black patients and those insured by Medicare and Medicaid (combined) waited longer before being listed. Patients with combined Medicare and Medicaid insurance, as well as those with Medicaid alone, were also more likely to die without ever being listed. Once listed, the time to transplant was slightly longer for women, but it did not differ by race/ethnicity or insurance. The early time period from diagnosis to listing for liver transplantation reveals unwanted variation related to demographics that jeopardizes overall fairness of organ allocation and needs to be further explored.
Figures

References
-
- Majeske RA. Transforming objectivity to promote equity in transplant candidate selection. Theoretical Medicine. 1996;17(1):45–59. - PubMed
-
- Milford EL. Organ transplantationn—barriers, outcomes, and evolving policies. Journal of the American Medical Association. 1998;280(13):1184–1185. - PubMed
-
- Navaneethan SD, Singh S. A systematic review of barriers in access to renal transplantation among African Americans in the United States. Clinical Transplantation. 2006;20(6):769–775. - PubMed
-
- Ubel PA, Loewenstein G. Public perceptions of the importance of prognosis in allocating transplantable livers to children. Medical Decision Making. 1996;16(3):234–241. - PubMed
-
- Ubel PA, Caplan AL. Geographic favoritism in liver transplantation—unfortunate or unfair? The New England Journal of Medicine. 1998;339(18):1322–1325. - PubMed
LinkOut - more resources
Full Text Sources
