

Metabolic syndrome and urologic diseases
- PMID: 21234260
- PMCID: PMC3020279
Metabolic syndrome and urologic diseases
Abstract
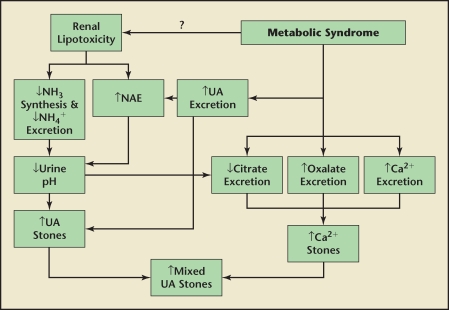
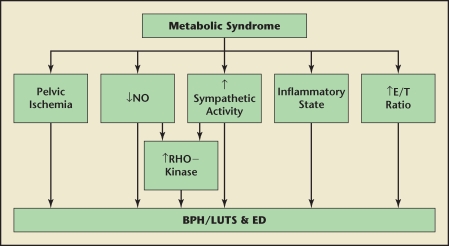
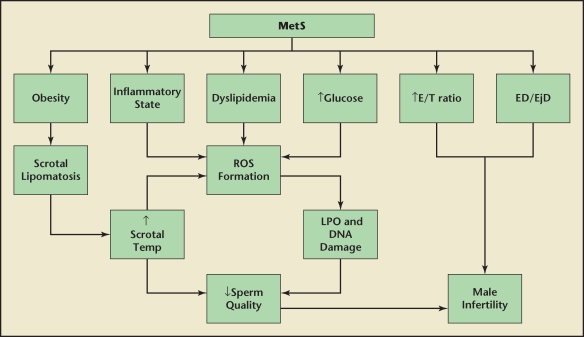
Metabolic syndrome (MetS) is a complex entity consisting of multiple interrelated factors including insulin resistance, central adiposity, dyslipidemia, endothelial dysfunction and atherosclerotic disease, low-grade inflammation, and in males, low testosterone levels. MetS has been linked to a number of urologic diseases including nephrolithiasis, benign prostatic hyperplasia and lower urinary tract symptoms, erectile dysfunction, male infertility, female incontinence, and prostate cancer. This article reviews the relationships between MetS and these entities. Urologists need to be cognizant of the impact that MetS has on urologic diseases as well as on overall patient health.
Keywords: Benign prostatic hyperplasia; Cardiovascular disease; Endothelial dysfunction; Hypogonadism; Insulin resistance; Lower urinary tract symptoms; Metabolic syndrome; Nephrolithiasis; Obesity.
Figures


References
-
- Alberti G. Introduction to the metabolic syndrome. Eur Heart J. 2005;7(suppl D):D3–D5.
-
- Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999–2000. JAMA. 2002;288:1723–1727. - PubMed
-
- Sturm R. Increases in clinically severe obesity in the United States, 1986–2000. Arch Intern Med. 2003;163:2146–2148. - PubMed
LinkOut - more resources
Full Text Sources